Acute Diverticulitis: Symptoms, Diagnosis, Treatment, and Prevention
What Is Acute Diverticulitis? A Complete Medical Overview
Acute diverticulitis is one of the most common gastrointestinal conditions affecting adults in Western countries, yet it remains widely misunderstood by patients and sometimes even underdiagnosed in clinical settings. If you or someone you care for has recently been diagnosed with acute diverticulitis — or if you're experiencing lower abdominal pain and wondering what's going on — this comprehensive guide will walk you through everything you need to know: what the condition is, what causes it, how it's diagnosed, how it's treated, and most importantly, how to prevent future episodes from occurring.
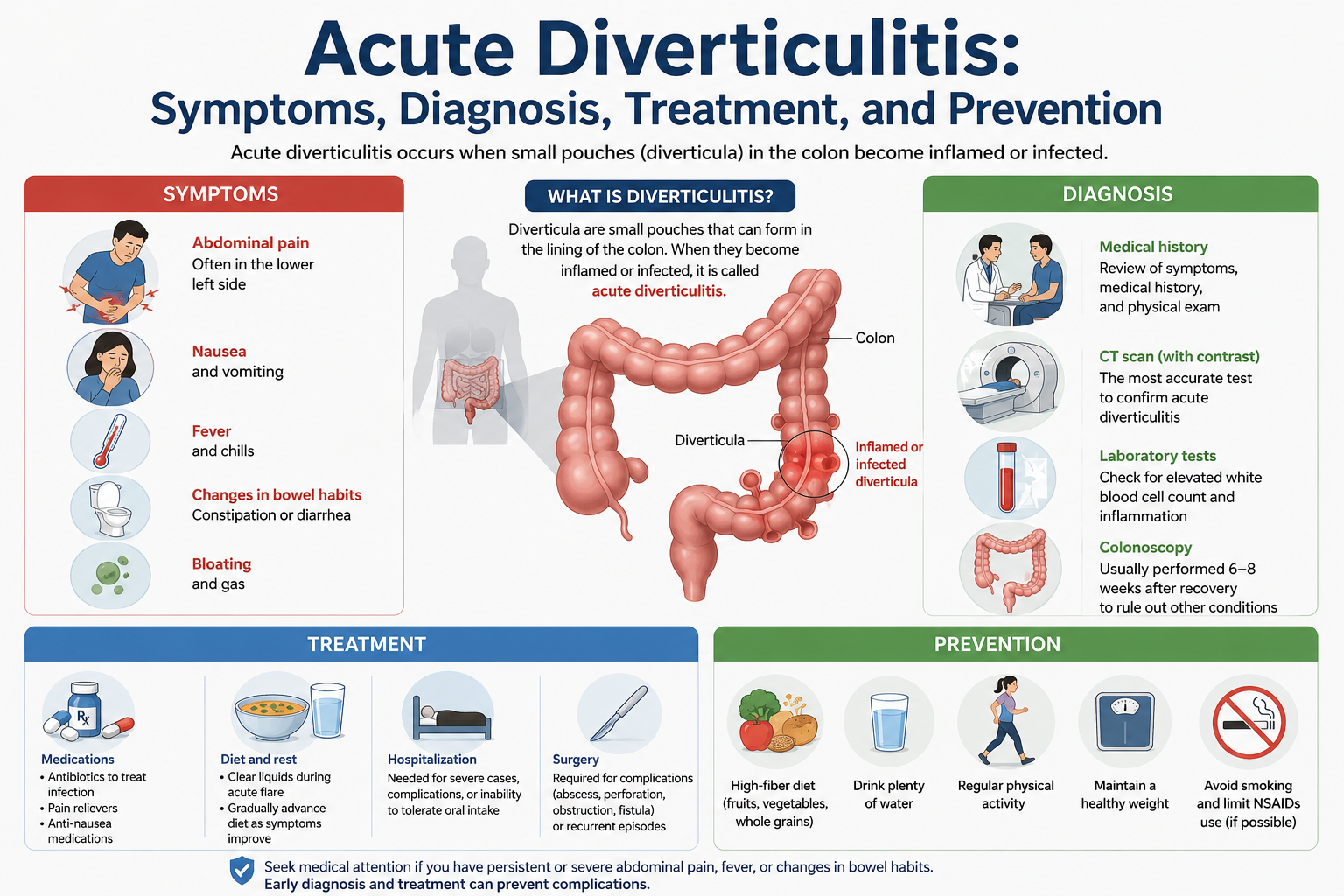
Understanding acute diverticulitis begins with understanding its precursor: diverticulosis. Diverticulosis is the condition in which small, bulging pouches called diverticula form in the walls of the colon, particularly in the sigmoid colon (the lower-left portion of the large intestine). These pouches develop at weak spots in the muscular wall of the colon, typically at points where blood vessels pass through. Diverticulosis itself is extremely common — estimates suggest that more than half of Americans over the age of 60 have it — and in most cases, it causes no symptoms at all. However, when one or more of these pouches become inflamed or infected, the result is diverticulitis. When this inflammation develops rapidly and severely, it is classified as "acute."
The Anatomy Behind Acute Diverticulitis
To truly understand acute diverticulitis, it helps to have a basic understanding of colon anatomy. The large intestine, or colon, is approximately five feet long and is responsible for absorbing water from indigestible food matter, then passing waste material out of the body. The colon is composed of several layers of tissue, including an inner mucosal layer, a muscular layer responsible for movement (peristalsis), and an outer serosal layer.
Diverticula — the plural of diverticulum — form when the inner layers of the colon push outward through weakened areas of the muscular wall. Think of it like a bicycle tire tube pushing through a small crack in the tire itself. These pouches are typically pea-sized, ranging from about 5 to 10 millimeters, though they can sometimes grow larger. In the United States and most Western nations, diverticula most commonly form in the sigmoid colon (the S-shaped portion in the lower left abdomen), while in Asian countries, right-sided colonic diverticulosis is more prevalent.
When fecal matter, bacteria, or other material becomes trapped in a diverticulum, it can trigger an inflammatory response. The bacteria that naturally live in the colon can multiply rapidly inside the trapped pocket, leading to localized infection. If the inflammation spreads to the peritoneum (the lining of the abdominal cavity), the condition becomes far more serious and potentially life-threatening.
Who Gets Acute Diverticulitis? Risk Factors and Epidemiology
Acute diverticulitis does not discriminate entirely by age, but it is significantly more common in older adults. Studies consistently show that the risk of developing diverticulitis increases with age, with the condition being relatively rare in people under 40. However, there has been a concerning trend in recent decades: younger adults — particularly those in their 30s and 40s — are being diagnosed with diverticulitis at increasing rates, with some research pointing to obesity, sedentary lifestyles, and poor dietary habits as contributing factors.
Here are the primary risk factors associated with acute diverticulitis:
Age: The most significant risk factor. Risk increases substantially after age 40 and continues to rise with each decade of life.
Diet low in fiber: A diet lacking adequate fiber is strongly associated with both diverticulosis formation and diverticulitis episodes. Fiber softens stool and supports healthy bowel movements, reducing pressure within the colon.
Obesity: Excess body weight, particularly abdominal obesity, significantly increases the risk of diverticulitis. Research published in major gastroenterology journals shows that obese individuals have a higher risk of both developing diverticulosis and experiencing acute episodes.
Physical inactivity: Regular physical activity appears to protect against diverticulitis. Sedentary lifestyles are associated with slower intestinal transit, increased intracolonic pressure, and higher risk of diverticular disease.
Smoking: Tobacco use has been linked to increased risk of complicated diverticulitis and poorer recovery outcomes.
Nonsteroidal anti-inflammatory drugs (NSAIDs): Regular use of NSAIDs such as ibuprofen, aspirin, and naproxen has been associated with a higher risk of diverticulitis complications, possibly by compromising the mucosal lining of the intestine.
Red meat consumption: Some epidemiological studies have found associations between high red meat intake and increased risk of diverticulitis, though the evidence is not as strong as with dietary fiber.
Genetics: Family history appears to play a role, with studies suggesting a genetic predisposition to developing diverticular disease.
Recognizing the Symptoms of Acute Diverticulitis
One of the most important aspects of acute diverticulitis management is early recognition of its symptoms. The condition can range from mild, uncomplicated inflammation to severe, life-threatening complications. The speed and appropriateness of treatment often depend on how quickly the condition is identified.
The hallmark symptom of acute diverticulitis is abdominal pain, typically located in the lower-left quadrant of the abdomen (corresponding to the sigmoid colon). This pain is usually described as a constant, dull ache that may worsen with movement or pressure. It can develop gradually over a period of days or come on more suddenly. In some patients, particularly those of Asian descent who are more likely to have right-sided diverticulosis, the pain may be felt on the right side, which can be confused with appendicitis.
Other common symptoms include:
Fever: A temperature above 100.4°F (38°C) is common in acute diverticulitis, reflecting the body's immune response to infection and inflammation.
Nausea and vomiting: These digestive symptoms often accompany the pain and may be severe enough to interfere with eating and drinking.
Changes in bowel habits: Patients may experience constipation (more common), diarrhea, or alternating patterns. In some cases, there may be a sensation of incomplete evacuation.
Bloating and gas: Abdominal distension and increased flatulence are frequently reported.
Rectal bleeding: While more commonly associated with uncomplicated diverticulosis, some patients with acute diverticulitis may notice blood in the stool.
Urinary symptoms: If the inflamed diverticulum is near the bladder or ureter, patients may experience frequent urination, pain with urination, or, in rare cases, pneumaturia (air in the urine), which can indicate a colovesical fistula.

Diagnosing Acute Diverticulitis
When a patient presents with symptoms suggestive of acute diverticulitis, clinicians use a combination of clinical assessment, laboratory tests, and imaging studies to confirm the diagnosis, assess severity, and rule out other conditions with similar presentations.
Clinical History and Physical Examination
The diagnostic process begins with a thorough medical history. The physician will ask about the nature, onset, and location of pain; associated symptoms; medication use; dietary habits; and any previous episodes of diverticulitis or diverticulosis. A history of known diverticular disease greatly increases the likelihood of a diverticulitis diagnosis.
Physical examination typically reveals tenderness in the lower-left abdomen. The physician will palpate the abdomen to check for guarding (involuntary muscular rigidity), rebound tenderness, and rigidity, all of which suggest more serious involvement. Bowel sounds may be decreased. In cases of perforation or peritonitis, the abdomen may be board-like and exquisitely tender to even light touch.
Laboratory Tests
Blood tests are an essential part of the diagnostic workup. The complete blood count (CBC) typically reveals an elevated white blood cell count (leukocytosis), indicating infection and inflammation. A C-reactive protein (CRP) level is particularly useful, as it tends to correlate well with disease severity and can help guide treatment decisions. Elevated CRP levels above 150 mg/L have been associated with a higher risk of complicated diverticulitis. Additional tests may include a metabolic panel to assess kidney function and electrolytes, especially if the patient is dehydrated from vomiting.
Urinalysis may be performed to rule out urinary tract infection as a cause of abdominal pain, and to look for signs of a colovesical fistula if urinary symptoms are present.
Imaging Studies
Imaging is the cornerstone of diverticulitis diagnosis and staging. CT (computed tomography) scan of the abdomen and pelvis with intravenous and oral contrast is the gold standard imaging modality for diagnosing acute diverticulitis. CT scan can confirm the diagnosis, identify complications (abscess, perforation, fistula, obstruction), assess the extent of inflammation, and help grade the severity using established classification systems such as the Hinchey classification.
CT findings in acute diverticulitis include thickening of the colon wall, pericolic fat stranding (inflammation around the colon), presence of diverticula, and possible air or fluid collections. The Hinchey classification grades diverticulitis from Stage I (pericolic abscess) through Stage IV (diffuse fecal peritonitis), helping surgeons and physicians determine appropriate management.
Ultrasound may be used as a first-line imaging tool in certain settings, particularly in pregnant patients (to avoid radiation) or when CT is not immediately available. MRI may be used in specific situations but is less commonly employed due to its cost and longer acquisition time.
The Hinchey Classification and Staging Acute Diverticulitis
Understanding how acute diverticulitis is classified helps explain why treatment approaches vary so widely between patients. The modified Hinchey classification system is the most widely used staging system for complicated acute diverticulitis:
Stage Ia — Pericolic abscess: A small abscess (collection of pus) forms adjacent to the affected diverticulum, surrounded by fatty tissue. This is considered a contained complication.
Stage Ib — Mesenteric or pericolic abscess: A larger abscess has formed within the mesentery (the tissue that connects the intestine to the abdominal wall).
Stage II — Pelvic abscess: The abscess has expanded into the pelvic cavity but remains walled off.
Stage III — Purulent peritonitis: The abscess has ruptured, spreading purulent (pus-containing) fluid throughout the peritoneal cavity.
Stage IV — Fecal peritonitis: A free perforation has occurred, allowing fecal material to leak into the peritoneal cavity. This is a surgical emergency with significant mortality risk.
Treatment of Acute Diverticulitis
The treatment of acute diverticulitis is highly individualized, depending on the severity of the episode, the presence of complications, the patient's overall health, and whether this is a first episode or recurrent disease. Broadly, treatment approaches are divided into conservative (non-surgical) and surgical management.
Conservative Treatment for Uncomplicated Diverticulitis
Approximately 75-80% of acute diverticulitis cases are uncomplicated (meaning no abscess, perforation, fistula, or obstruction), and the vast majority of these can be managed conservatively without hospitalization. Key components of outpatient management include:
Dietary modification: During an acute episode, a liquid or low-fiber diet is typically recommended to reduce the workload on the colon and allow the inflamed tissue to rest. As symptoms resolve (usually over 2-4 days), solid foods are gradually reintroduced. Contrary to older beliefs, a clear liquid diet is not always necessary for mild, uncomplicated diverticulitis.
Antibiotics: Historically, antibiotics were considered the cornerstone of diverticulitis treatment. However, recent well-designed clinical trials — including the landmark AVOD and DIABOLO studies — have demonstrated that antibiotics may not be necessary for mild, uncomplicated diverticulitis in otherwise healthy patients. Current guidelines increasingly recommend selective use of antibiotics, reserving them for immunocompromised patients, those with significant comorbidities, patients with high fever, or those who fail to improve without antibiotics. When prescribed, typical regimens include a combination of a fluoroquinolone (such as ciprofloxacin) or trimethoprim-sulfamethoxazole plus metronidazole, or a single broad-spectrum agent such as amoxicillin-clavulanate, taken for 7-10 days.
Pain management: Acetaminophen (paracetamol) is the preferred analgesic for pain control during an acute episode. NSAIDs are generally avoided due to their potential to increase the risk of perforation and other complications.
Rest and hydration: Adequate hydration is essential, particularly if the patient has experienced nausea and vomiting. Oral rehydration is preferred; intravenous fluids may be needed in more severe cases or when oral intake is not possible.
Hospital-Based Treatment for Complicated Diverticulitis
Patients with complicated diverticulitis, those who cannot tolerate oral intake, those with severe systemic symptoms, or those with significant comorbidities typically require hospitalization. Inpatient management includes:
IV antibiotics and fluids: Broad-spectrum intravenous antibiotics covering gram-negative bacteria and anaerobes are administered. Common regimens include piperacillin-tazobactam, ticarcillin-clavulanate, or a combination of ceftriaxone plus metronidazole.
Percutaneous drainage: For Hinchey Stage I and Stage II abscesses (those larger than 3-4 cm), CT-guided or ultrasound-guided percutaneous drainage by an interventional radiologist can effectively drain the abscess, allowing the patient to avoid emergency surgery. A drainage catheter is placed through the skin directly into the abscess cavity, and antibiotics are continued.
Bowel rest: Patients may be kept nil per os (NPO — nothing by mouth) initially, particularly if surgery is being considered or if there is significant peritoneal irritation.
Surgical Treatment
Surgical intervention is required in specific situations: emergency surgery for Hinchey Stage III/IV peritonitis, failure of conservative management, recurrent episodes causing significant impact on quality of life, or suspicion of underlying malignancy.
Emergency surgery (Hartmann's procedure): For perforated diverticulitis with peritonitis, the standard surgical approach has traditionally been a Hartmann's procedure — resection of the sigmoid colon, creation of a temporary colostomy, and closure of the rectal stump. This allows for source control while avoiding a dangerous primary anastomosis in a contaminated field. However, primary anastomosis (reconnecting the bowel) with or without a diverting ileostomy is increasingly being performed in selected patients with good results.
Elective sigmoid colectomy: This is the planned surgical removal of the sigmoid colon (the most commonly affected segment) for recurrent or complicated diverticulitis. It can be performed laparoscopically (minimally invasive), which typically results in shorter hospital stays, less pain, and faster recovery compared to open surgery. The decision to proceed with elective surgery is made on a case-by-case basis, considering the number and severity of previous attacks, the patient's age, overall health, and preferences.

Complications of Acute Diverticulitis
When left untreated or when treatment is inadequate, acute diverticulitis can lead to a range of serious complications that significantly increase morbidity and mortality. Understanding these potential complications underscores the importance of prompt diagnosis and appropriate treatment.
Abscess formation: One of the most common complications, occurring when pus collects near the inflamed diverticulum. Small abscesses may resolve with antibiotics alone, while larger ones require drainage.
Perforation: A rupture of the diverticulum or surrounding tissue that allows intestinal contents to leak into the abdominal cavity, causing peritonitis. This is a surgical emergency associated with significant mortality if not treated rapidly.
Fistula formation: Chronic inflammation can erode through adjacent structures, creating abnormal connections (fistulas) between the colon and other organs. Colovesical fistulas (between colon and bladder) are the most common, presenting with recurrent urinary tract infections, pneumaturia (air bubbles in urine), or fecaluria (fecal material in urine). Colovaginal and colocutaneous fistulas can also occur.
Bowel obstruction: Repeated episodes of diverticulitis can lead to scarring and narrowing (stricture) of the colon, causing partial or complete bowel obstruction. Symptoms include cramping, bloating, constipation, and sometimes vomiting.
Sepsis: Severe infection can overwhelm the body's immune response, leading to systemic inflammatory response syndrome (SIRS) and sepsis, a potentially life-threatening condition requiring intensive care management.
Recovery and Long-Term Management After an Episode
Recovery from an uncomplicated episode of acute diverticulitis typically takes 2-4 weeks. Most patients experience significant improvement in symptoms within 2-3 days of starting treatment. However, the resolution of the acute episode is just the beginning of long-term diverticular disease management.
Following recovery, it is essential for patients to follow up with their physician or gastroenterologist. A colonoscopy is typically recommended 6-8 weeks after an episode of acute diverticulitis to rule out underlying colorectal cancer (which can sometimes present with similar CT findings) and to fully assess the colon. This is particularly important for patients experiencing their first episode or those with atypical features.
Dietary changes form the cornerstone of long-term prevention. Transitioning to a high-fiber diet (25-35 grams per day) is consistently recommended to reduce intracolonic pressure and promote healthy bowel function. Rich sources of dietary fiber include fruits, vegetables, whole grains, legumes, and nuts. Adequate hydration (6-8 glasses of water daily) is equally important to support fiber's benefits. Contrary to popular myth that was debunked by multiple studies, there is no scientific evidence that eating nuts, seeds, popcorn, or corn increases the risk of diverticulitis flares — patients do not need to avoid these foods.
Regular physical activity — at least 30 minutes of moderate exercise most days of the week — is associated with a lower risk of diverticulitis recurrence. Weight management is also important, as obesity is a significant risk factor.
Some evidence supports the use of mesalazine (mesalamine) and rifaximin (a non-absorbable antibiotic) in the prevention of recurrent diverticulitis, though the evidence base is still evolving. Probiotics have also been studied for their potential role in modulating the gut microbiome and reducing inflammation, with promising but inconclusive results.
Preventing Acute Diverticulitis: Evidence-Based Strategies
While not every episode of acute diverticulitis is preventable, especially in those with extensive diverticulosis, a number of evidence-based lifestyle and dietary modifications can meaningfully reduce the frequency and severity of episodes:
Increase dietary fiber: Multiple large-scale studies, including the landmark Health Professionals Follow-Up Study, have demonstrated that higher fiber intake is associated with a significantly reduced risk of diverticular disease. Aim for 25-35g of fiber per day from a variety of plant-based sources.
Stay physically active: Regular vigorous exercise (running, cycling, swimming) appears particularly protective. Physical activity promotes gut motility and reduces intracolonic pressure.
Maintain a healthy weight: Achieving and maintaining a healthy BMI reduces intraabdominal pressure and systemic inflammation.
Quit smoking: Smoking cessation reduces the risk of diverticulitis complications and improves overall gastrointestinal health.
Limit red meat: Reducing consumption of processed and red meats in favor of poultry, fish, and plant-based proteins may reduce risk based on epidemiological data.
Limit NSAID use: If you need pain relief, acetaminophen is preferred over NSAIDs such as ibuprofen for regular use.
Stay well hydrated: Adequate fluid intake keeps stool soft and supports regular bowel movements, reducing pressure on the colon wall.
When to Seek Immediate Medical Attention
Knowing when to seek urgent medical care for potential acute diverticulitis can be lifesaving. You should seek emergency medical attention immediately if you experience any of the following:
Severe abdominal pain that is getting worse rapidly; high fever (above 102°F / 39°C) combined with abdominal pain; inability to keep any liquids down due to vomiting; bloody stool or significant rectal bleeding; abdominal rigidity or board-like hardness; lightheadedness or fainting; signs of sepsis (rapid heart rate, confusion, rapid breathing).
Even for milder symptoms, you should contact your doctor promptly — within 24 hours — if you experience new left lower abdominal pain with fever, especially if you have known diverticular disease. Early treatment of uncomplicated diverticulitis dramatically reduces the risk of progression to complicated disease.
Frequently Asked Questions About Acute Diverticulitis
Can acute diverticulitis go away on its own?
Mild cases of uncomplicated acute diverticulitis may sometimes resolve without antibiotic treatment, particularly in otherwise healthy individuals. However, this should never be assumed. Any episode of diverticulitis should be evaluated by a physician to assess its severity and determine the most appropriate course of action. Untreated diverticulitis risks progressing to serious complications including perforation and peritonitis.
Is acute diverticulitis the same as appendicitis?
No. Appendicitis is inflammation of the appendix and typically causes pain in the lower-right abdomen, while diverticulitis most commonly causes pain in the lower-left abdomen. However, right-sided diverticulitis (more common in Asian populations) and certain atypical presentations of appendicitis can overlap in location. CT scan is the most reliable way to distinguish between the two.
How long does an episode of acute diverticulitis last?
With appropriate treatment, most uncomplicated episodes resolve within 2-7 days. Complicated cases requiring hospitalization, drainage, or surgery may take several weeks. After the acute phase, some residual tenderness or bowel irregularity may persist for 4-6 weeks.
Can you eat normally after recovering from diverticulitis?
Yes, but with modifications. Long-term dietary changes — particularly increasing fiber and fluid intake — are recommended to prevent recurrence. During the acute phase, a bland, low-fiber diet is recommended, but after full recovery, patients are typically advised to gradually increase fiber intake to high levels.
Does diverticulitis increase the risk of colon cancer?
There is no direct causal relationship between diverticulitis and colon cancer. However, because the symptoms can sometimes overlap and because some colorectal cancers can be missed on CT imaging, colonoscopy is typically recommended after recovery from a first episode to ensure the colon is fully evaluated and to rule out malignancy.
Conclusion
Acute diverticulitis is a common, often painful, and potentially serious condition that affects millions of people worldwide. Understanding its causes, recognizing its symptoms early, seeking timely medical attention, and following evidence-based treatment and prevention strategies are the keys to managing this disease effectively. While diverticulitis can be frightening, the vast majority of episodes are uncomplicated and respond well to conservative management. With appropriate lifestyle modifications — particularly adopting a high-fiber diet, staying active, and maintaining a healthy weight — many patients can significantly reduce their risk of recurrent episodes and live comfortably despite having diverticular disease.
If you believe you may be experiencing an episode of acute diverticulitis, do not delay in seeking medical care. Early evaluation and treatment are your best protection against complications. Work closely with your gastroenterologist or primary care physician to develop a personalized management plan, and take proactive steps today to protect your long-term digestive health.