Bowel Obstruction: Causes, Diagnosis, and Treatment Explained
2026-05-115 views5 min read
Bowel Obstruction: Causes, Diagnosis, and Treatment Explained
A bowel obstruction is one of the most common abdominal emergencies seen in hospitals worldwide. Despite being a well-understood condition medically, it continues to catch patients and their families off guard — largely because the symptoms can mimic other, less serious digestive problems. Understanding what a bowel obstruction actually is, what causes it, how it is diagnosed, and how it is treated can help you navigate this frightening situation with knowledge and confidence.
This article takes a comprehensive, evidence-based look at bowel obstruction — from its underlying biology to its clinical management.
Defining Bowel Obstruction
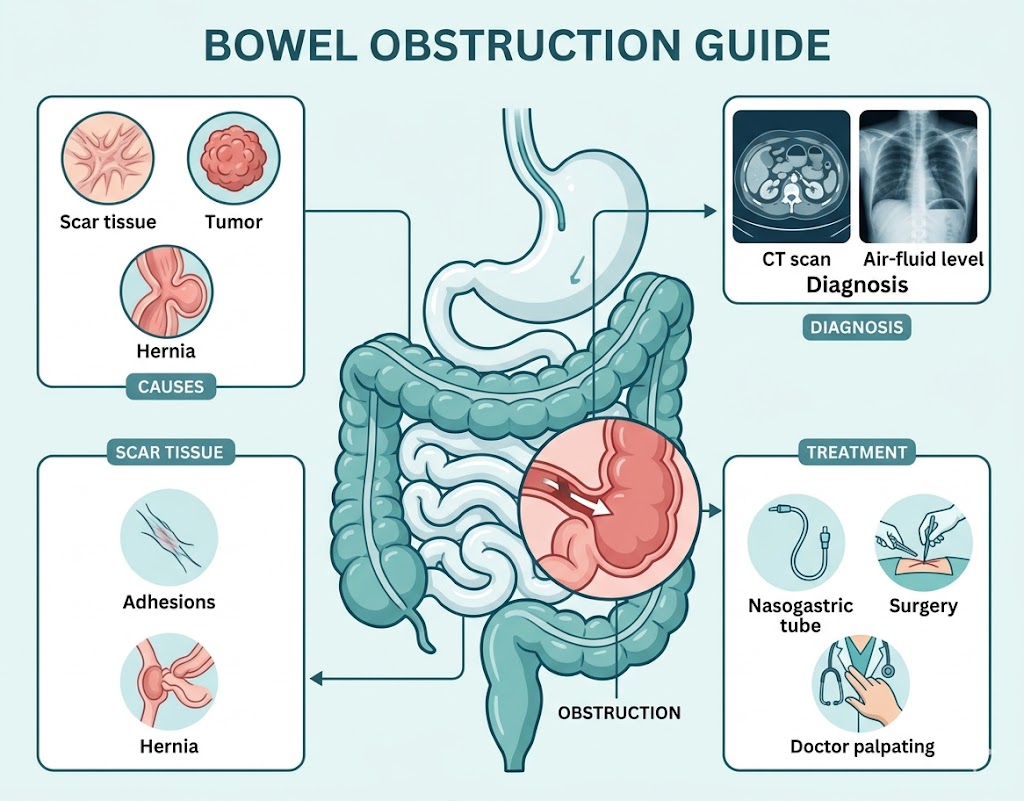
A bowel obstruction occurs when the normal passage of intestinal contents — digested food, fluid, gas, and waste — is partially or completely blocked somewhere along the gastrointestinal (GI) tract. The blockage can affect either the small intestine (small bowel obstruction, or SBO) or the large intestine (large bowel obstruction, or LBO).
When flow is impeded, several dangerous processes begin to unfold simultaneously. Gas and fluid accumulate behind the blockage, causing distension and increasing intraluminal pressure. The intestinal wall, stretched beyond normal limits, begins to lose its ability to absorb fluid — instead, it starts leaking fluid into the intestinal lumen. As pressure continues to rise, blood supply to the bowel wall may be compromised, leading to ischemia and eventually necrosis (tissue death). If the bowel perforates, life-threatening peritonitis and sepsis can develop within hours.
This cascade explains why bowel obstruction is classified as a medical emergency that demands rapid evaluation and treatment.
The Two Major Categories of Bowel Obstruction
Before exploring causes, it is essential to understand the two fundamental categories of bowel obstruction, because they have fundamentally different mechanisms:
Mechanical Obstruction
Mechanical obstruction involves a physical barrier — something that physically blocks the lumen of the intestine. This barrier can be:
- Inside the bowel lumen (intraluminal): a foreign body, impacted stool (fecal impaction), a large gallstone (gallstone ileus), or a large polyp
- Within the bowel wall (intramural): a tumor, stricture from Crohn's disease, scar tissue from radiation, or intussusception (where one segment of bowel telescopes into another)
- Outside the bowel (extrinsic): adhesions (bands of scar tissue), hernias, volvulus (twisting), or external compression from a tumor
Mechanical obstructions require the physical barrier to be removed or bypassed, either surgically or endoscopically.
Functional Obstruction (Ileus and Pseudo-obstruction)
Functional obstruction has no physical barrier — instead, the bowel's own muscles stop working. The intestinal wall becomes paralyzed and motility ceases, causing the same buildup of gas and fluid as a mechanical obstruction.
Ileus is the most common form, typically occurring after abdominal surgery. It is usually temporary and resolves as normal bowel function returns.
Colonic pseudo-obstruction (Ogilvie's syndrome) is a more severe and potentially dangerous variant in which the colon massively dilates without physical obstruction. It most commonly occurs in hospitalized elderly patients with serious underlying illness.
Causes of Bowel Obstruction: A Detailed Breakdown
Small Bowel Obstruction Causes
Adhesions (scar tissue): The most common cause of SBO in developed countries, accounting for approximately 60-70% of all small bowel obstructions. Adhesions form after abdominal or pelvic surgery as part of the healing process — fibrous bands develop between loops of bowel or between bowel and the abdominal wall, creating potential chokepoints. Previous appendectomy, hysterectomy, cesarean section, and colorectal surgery are particularly associated with adhesion formation.
Hernias: The second most common cause of SBO worldwide. An inguinal hernia (groin hernia), femoral hernia, umbilical hernia, or incisional hernia can trap a loop of bowel, cutting off its blood supply in a process called incarceration and strangulation. Strangulated hernias are surgical emergencies.
Crohn's disease: Chronic inflammation of the small intestine in Crohn's disease leads to thickening and scarring of the bowel wall over time, progressively narrowing the intestinal lumen. Patients with long-standing Crohn's disease are at significant risk for recurrent partial obstructions.
Tumors: Malignant or benign tumors of the small intestine can cause obstruction, though this is less common than in the large intestine. Metastatic cancers (particularly ovarian, colorectal, and gastric cancer) can also spread to the small bowel and cause obstruction.
Intussusception: More common in children than adults, intussusception occurs when one section of bowel "telescopes" into the adjacent section, like a finger being pushed into a glove. In adults, a lead point (such as a tumor or polyp) is almost always responsible.
Volvulus of the small bowel: Though less common than colonic volvulus, the small bowel can twist on its mesenteric axis, cutting off blood supply rapidly.
Large Bowel Obstruction Causes
Colorectal cancer: The leading cause of large bowel obstruction in Western countries. A growing tumor can progressively narrow the colon lumen until it becomes completely obstructed. Obstruction is sometimes the first presentation of colorectal cancer in patients who have had no prior symptoms.
Diverticular disease: Repeated episodes of diverticulitis (inflammation of diverticula, which are small pouches in the colon wall) can lead to scarring and stricture formation that eventually obstructs the colon. Acute diverticulitis can also cause acute obstruction through inflammation and edema.
Volvulus: A volvulus occurs when a segment of colon twists around its mesenteric axis. The sigmoid colon is most frequently involved (sigmoid volvulus), followed by the cecum (cecal volvulus). Volvulus can cut off the blood supply rapidly and progress to strangulation and perforation.
Ogilvie's syndrome (pseudo-obstruction): As described above, this functional condition causes massive colonic dilation without a physical blockage. It is associated with serious systemic illness, electrolyte abnormalities, narcotic use, and immobility.
Fecal impaction: In elderly, debilitated, or chronically constipated patients, impacted stool can become hard and immovable, physically obstructing the colon.
How Bowel Obstruction Is Diagnosed
When a patient presents with symptoms of bowel obstruction, the diagnostic process moves quickly. The goal is to confirm the obstruction, identify its location and severity, determine whether blood supply to the bowel is compromised, and find the underlying cause.
History and Physical Examination
The doctor will ask detailed questions about:
- Onset and character of abdominal pain
- Vomiting (what it looks like and how frequently)
- Last bowel movement and passage of gas
- History of abdominal surgery
- Known hernias, Crohn's disease, or colorectal cancer
- Current medications (especially opioids)
On physical examination, the doctor will assess for abdominal distension, tenderness, rigidity (which suggests peritonitis), and bowel sounds. A digital rectal exam may be performed to assess for impacted stool, blood, or a rectal mass.
Laboratory Tests
Blood tests ordered in suspected bowel obstruction include:
- Complete blood count (CBC): Elevated white blood cell count suggests infection, ischemia, or perforation
- Basic metabolic panel: Electrolyte abnormalities (particularly hypokalemia) can contribute to ileus; kidney function assesses dehydration severity
- Lactate level: Elevated lactate suggests bowel ischemia and is a marker of poor outcomes
- Liver function tests and lipase: To exclude other causes of abdominal pain
- Blood cultures: If fever or sepsis is suspected
Imaging
Plain abdominal X-rays: Still the first-line imaging test in many settings. In bowel obstruction, X-rays show:
- Dilated loops of bowel (small bowel >3 cm diameter, large bowel >6 cm diameter)
- Air-fluid levels (horizontal lines at different heights within the same bowel loop, caused by gas sitting above pooled fluid)
- "Stack of coins" appearance in small bowel obstruction (caused by prominent mucosal folds called plicae circulares)
- Absent colonic gas in complete obstruction
CT scan of the abdomen and pelvis with intravenous contrast: This is the gold-standard imaging study for bowel obstruction. CT provides information that plain X-rays simply cannot:
- Precise location of the transition point (where dilated bowel meets collapsed bowel)
- Identification of the cause (adhesion, hernia, tumor, volvulus)
- Assessment of bowel wall enhancement to detect ischemia
- Presence of pneumatosis (gas in the bowel wall — sign of necrosis)
- Free air in the abdomen (sign of perforation)
- Presence of ascites or peritoneal findings
Contrast enema: In suspected large bowel obstruction, a water-soluble contrast enema (not barium, to avoid contaminating the abdominal cavity if perforation occurs) can define the level of obstruction and sometimes identify the cause.
Water-soluble contrast follow-through: In partial small bowel obstructions managed conservatively, oral water-soluble contrast may be given. If contrast reaches the colon within 24 hours, it is predictive that the obstruction will resolve without surgery — and the contrast itself may have a therapeutic effect.
Treatment of Bowel Obstruction
Initial Stabilization
All patients admitted with bowel obstruction receive initial stabilization regardless of whether surgery will ultimately be needed:
Intravenous access and fluid resuscitation: Patients are often severely dehydrated from vomiting and third-spacing of fluid. IV fluids (typically normal saline or lactated Ringer's) are given to restore circulating volume and correct electrolyte imbalances.
Nasogastric (NG) tube: A thin tube passed through the nose into the stomach decompresses the proximal GI tract, relieving nausea and vomiting and reducing the risk of aspiration. It also rests the bowel and reduces distension.
Nil by mouth: The patient is kept from eating or drinking to rest the bowel and prepare for possible surgery.
Urinary catheter: A catheter is placed to monitor urine output as a guide to fluid resuscitation.
Monitoring: Vital signs, oxygen saturation, urine output, and repeat abdominal examinations are performed frequently to watch for deterioration.
Non-Surgical Management
Many partial small bowel obstructions — especially adhesive SBO — can be treated successfully without surgery. Studies show that 65-80% of adhesive SBO cases resolve with conservative management within 24-72 hours.
The decision to manage conservatively versus surgically depends on:
- Whether the obstruction is complete or partial
- Whether there are any signs of strangulation (fever, elevated lactate, severe pain, peritoneal signs)
- The underlying cause
- The patient's response to treatment over time
Conservative management involves IV fluids, NG tube decompression, nil by mouth, and close monitoring. The patient is reassessed regularly, and if they do not improve or worsen, surgery is escalated promptly.
Surgical Management
Surgery is required for:
- Complete bowel obstructions that do not resolve with conservative management
- Any obstruction with signs of strangulation or bowel ischemia
- Closed-loop obstruction (a particularly dangerous configuration where bowel is blocked at two points simultaneously, rapidly building pressure)
- Bowel perforation
- Hernias causing obstruction
- Volvulus requiring bowel resection
The type of surgery depends on the cause and extent of damage:
Adhesiolysis: Cutting and releasing adhesive bands. Can often be done laparoscopically (keyhole surgery) if the bowel is not too distended.
Hernia repair: The incarcerated bowel is reduced (gently pushed back) and the hernia defect is repaired. If the bowel is strangulated and necrotic, the affected segment is resected.
Bowel resection and anastomosis: The obstructed or necrotic segment of bowel is removed and the two ends are joined together (anastomosis). In some cases, particularly with large bowel obstruction and peritonitis, a temporary colostomy is created rather than an anastomosis.
Detorsion of volvulus: A sigmoid volvulus can sometimes be "untwisted" using a colonoscope (flexible endoscope) as a temporizing measure, but definitive surgical treatment (sigmoid resection) is usually recommended.
Endoscopic stenting: Self-expanding metal stents placed colonoscopically can relieve large bowel obstruction caused by colorectal cancer, either as a bridge to elective surgery or as definitive palliation in patients who are not surgical candidates.
Complications of Bowel Obstruction
Without timely treatment, bowel obstruction can lead to:
Bowel ischemia and necrosis: Loss of blood supply causes the bowel wall to die, making it susceptible to bacterial invasion.
Perforation: A dead or severely ischemic bowel can rupture, spilling intestinal contents into the peritoneal cavity.
Peritonitis: Infection of the peritoneal cavity following perforation, causing severe systemic illness.
Sepsis: Bacteria entering the bloodstream from a perforated bowel can cause sepsis, multi-organ failure, and death if not treated rapidly with antibiotics and source control (surgery).
Short bowel syndrome: Extensive bowel resection may leave insufficient small intestine to absorb adequate nutrition, requiring long-term parenteral (IV) nutrition.
Recurrence: Particularly after adhesive SBO, the risk of future obstructions is significant — estimated at 10-30% over a patient's lifetime.
Prognosis and Recovery
The prognosis for bowel obstruction depends heavily on how quickly it is identified and treated, and whether complications such as strangulation or perforation have occurred.
For uncomplicated partial SBO treated conservatively, outcomes are excellent. For surgical cases without complications, mortality is low (1-3%). However, when strangulation, perforation, or sepsis are present, mortality rises significantly, particularly in elderly patients.
Recovery after surgery for bowel obstruction typically involves 3-7 days in the hospital, with gradual resumption of oral intake as bowel function returns. Full recovery at home may take several weeks, and patients are advised to watch carefully for any recurrence of symptoms.
Conclusion
Bowel obstruction is a complex medical condition with multiple causes, presentations, and treatment paths. What unifies all cases is the need for prompt medical evaluation — the faster the condition is identified and managed, the better the outcomes. If you or someone you know develops severe abdominal pain, vomiting, abdominal swelling, and inability to pass gas or stool, do not wait: seek emergency care immediately. With proper treatment, most people with bowel obstruction make a full recovery and go on to live healthy, normal lives.