Bowel Obstruction Symptoms: A Step-by-Step Guide to Recognition
2026-05-1111 views5 min read
Bowel Obstruction Symptoms: A Step-by-Step Guide to Recognition
When someone develops a bowel obstruction, the body sends a series of escalating signals — signals that, if recognized early, can prompt life-saving action. Yet the challenge for patients, family members, and even primary care providers is that these symptoms can begin subtly and overlap with more common, benign conditions like gastroenteritis, constipation, or irritable bowel syndrome.
This guide takes a step-by-step approach to understanding bowel obstruction symptoms — what they feel like at each stage, how to tell them apart from ordinary digestive complaints, and when the situation demands emergency intervention. Whether you are someone with risk factors for obstruction, a caregiver, or simply someone who wants to be better informed, this guide provides the knowledge you need.
Understanding the Context: Why Symptoms Happen
Before walking through the symptoms, it helps to understand why they occur. A bowel obstruction blocks the normal movement of intestinal contents. When this happens:
The intestinal muscles do not "give up" immediately — they continue contracting forcefully to try to push contents past the blockage. This muscular effort creates the waves of cramping pain.
Gas and fluid accumulate behind the blockage, because there is nowhere for them to go. This creates the bloating, distension, and pressure sensation.
The body tries to reverse the flow when forward movement is impossible. This produces nausea and eventually vomiting.
As pressure builds and the bowel wall stretches, blood flow to the tissue becomes compromised. This is when the situation becomes dangerous.
Each symptom maps directly to one of these biological processes, which is why understanding the mechanism makes the symptoms easier to recognize and remember.
Stage 1: The Early Warning Signs
In the initial phase of a bowel obstruction — often the first few hours — symptoms may be easy to dismiss. This is precisely why they deserve close attention, especially in people with known risk factors.
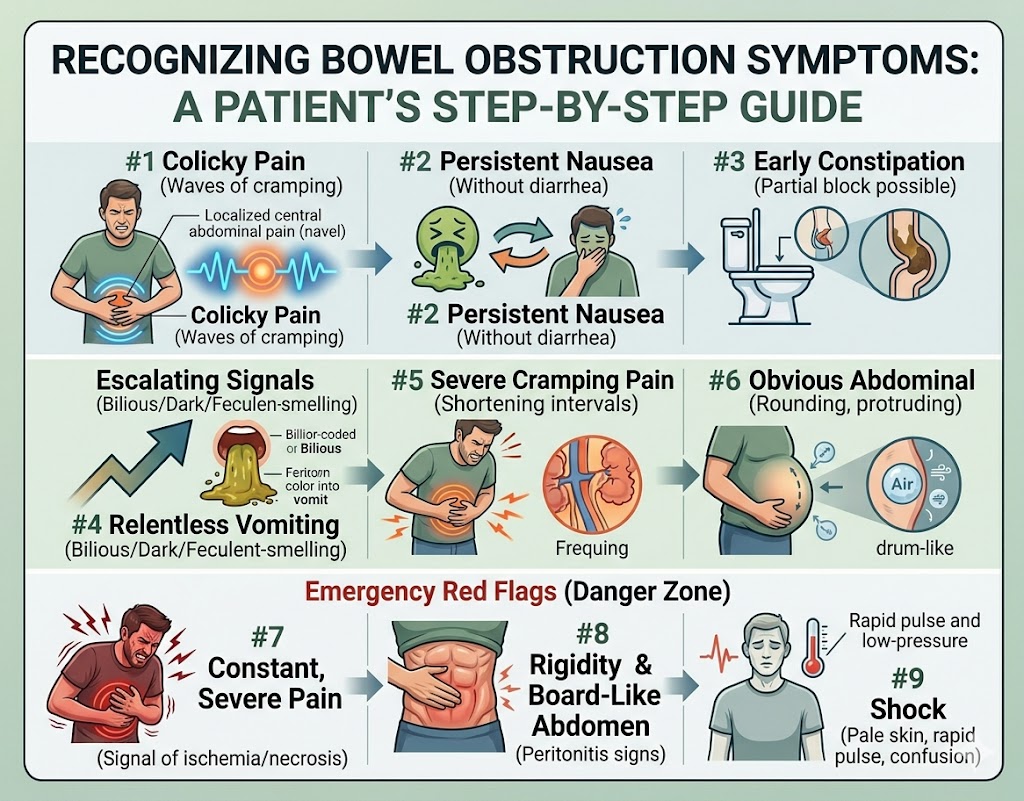
Early Crampy Abdominal Pain
The first symptom most people notice is pain that comes in waves. Unlike the steady, constant ache of appendicitis or the sharp localized pain of kidney stones, early bowel obstruction pain is typically:
Colicky — it surges, peaks, and then temporarily eases
Located around the navel or in the central abdomen (for small bowel obstruction) or the lower abdomen (for large bowel obstruction)
Separated by intervals of relative comfort, especially early on
Synchronized with audible or felt gurgling as the gut tries to push past the blockage
Many patients initially mistake this for "bad gas" or a stomach bug. The key distinguishing feature is persistence: this pain does not resolve with position changes, passing gas, or antacids.
Mild Nausea
Nausea is almost always present from the start. It is often mild initially — a background queasiness rather than acute sickness. The patient may feel "off" but not yet in distress. This nausea tends to worsen progressively rather than fluctuate, unlike the nausea of food poisoning which often comes in waves and resolves.
Early Constipation and Difficulty Passing Gas
Patients may notice that they are not passing gas as easily or as frequently as usual. Early in an obstruction, this may be subtle — the patient may pass a small amount of stool or gas from the segment of bowel below the obstruction, giving false reassurance. Over time, this slows and stops entirely.
Loss of Appetite
Along with the nausea, the idea of eating becomes unappealing. The body is protecting itself — adding more food to a blocked system would only worsen the situation.
Stage 2: The Middle Phase — Symptoms Intensify
If the obstruction is not recognized and treated during Stage 1, symptoms progress and the patient enters a more obvious clinical picture.
Worsening and More Constant Abdominal Pain
The pain transitions from intermittent and colicky to more persistent. The intervals of relief shorten. The location may expand or shift as more of the bowel becomes involved. Pressing on the abdomen may now produce noticeable tenderness.
At this stage, the patient is usually significantly uncomfortable and unlikely to mistake the situation for simple indigestion.
Active Vomiting
Vomiting typically begins in this stage (for small bowel obstruction) or intensifies. The character of the vomit provides important diagnostic clues:
Bilious (greenish-yellow) vomiting: Indicates bile is present, meaning the obstruction is below the stomach but relatively high in the small intestine. This is a significant symptom.
Dark brown or feculent-smelling vomit: Suggests the obstruction is further down, and that intestinal bacteria have had time to act on accumulated fluid. This is a red flag for a more advanced or lower obstruction.
Repeated vomiting with little relief: Unlike vomiting from food poisoning, which typically provides some temporary relief, vomiting from bowel obstruction is relentless because the upstream obstruction keeps feeding the stomach with backed-up intestinal contents.
Visible Abdominal Distension
The abdomen becomes noticeably swollen. The patient may observe that their clothes fit more tightly or that their abdomen appears rounded and protrudes more than usual. When tapped (percussed), the abdomen makes a drum-like, hollow sound — a sign of air-filled loops of bowel.
This distension is particularly pronounced in large bowel obstructions and those involving the lower small intestine, where a greater length of bowel is dilated behind the blockage.
Hyperactive Bowel Sounds
A person lying still or a healthcare provider using a stethoscope may hear unusually loud, high-pitched gurgling sounds — like rushing water through a narrow pipe. These hyperactive bowel sounds (borborygmi) reflect the bowel's futile attempts to push contents past the obstruction.
Some patients find that they can actually hear these sounds without a stethoscope, especially when the abdomen is quiet. The sound may be described as a loud rushing or rumbling noise occurring in bursts.
Progressive Dehydration Symptoms
Persistent vomiting and the inability to take in fluids by mouth lead to dehydration. Signs include:
Dry mouth and increased thirst
Decreased frequency of urination with darker-colored urine
Lightheadedness or dizziness, especially when standing
A feeling of weakness or fatigue
Rapid heartbeat (the heart tries to compensate for low circulating blood volume)
Dehydration compounds the clinical picture and requires treatment with intravenous fluids.
Stage 3: The Danger Zone — When Symptoms Signal Emergency
Stage 3 represents complications: strangulation of the bowel (loss of blood supply), perforation (rupture), and peritonitis (infection of the abdominal cavity). These are all surgical emergencies.
The Shift from Colicky to Constant, Severe Pain
One of the most important clinical observations in bowel obstruction is the transition from colicky (intermittent wave-like) pain to constant, severe pain. This transition suggests that the bowel wall is no longer just obstructed — it is ischemic (deprived of blood) or necrotic (dying).
The pain becomes:
Continuous and relentless, without the intervals of relief seen earlier
More severe and out of proportion to what the patient had been experiencing
Associated with extreme tenderness when the abdomen is touched
Sometimes radiating to the back or to the shoulder (in cases of perforation with diaphragm irritation)
If you or someone you are caring for experiences this transition, emergency services must be called immediately.
Fever
Fever above 38°C (100.4°F) in the context of abdominal pain and obstruction symptoms is a serious warning sign. It suggests one of the following is occurring:
- Bacterial translocation (bacteria leaking from the distended bowel into the bloodstream)
- Perforation and spillage of bowel contents into the abdominal cavity
- Peritonitis (infection of the peritoneal lining)
The higher and more rapidly rising the fever, the more urgent the situation.
Rigid, Board-Like Abdomen
Normally, the abdomen has some give to it — pressing in produces mild discomfort at most. In peritonitis, the abdominal wall muscles involuntarily contract to protect the inflamed underlying structures. This creates a rigid, board-like abdomen that is exquisitely tender to the touch. Even light pressure causes severe pain.
This finding, known as peritonism, is a late and serious sign that requires immediate surgical intervention.
Absent Bowel Sounds
As the bowel becomes progressively ischemic and fatigued, or once peritonitis has developed, bowel sounds disappear entirely. The abdomen becomes eerily silent when listened to with a stethoscope — a sign of ileus (paralysis) secondary to peritonitis or advanced obstruction.
Signs of Shock
In the most severe cases, the patient may develop signs of circulatory shock:
Pale, gray, or ashen skin
Cold, clammy extremities
Very rapid, weak pulse
Extreme low blood pressure
Confusion or altered mental status
Rapid breathing
These signs indicate systemic sepsis or massive volume loss and represent an immediate life threat. Call emergency services without delay.
Bowel Obstruction vs. Common Digestive Complaints: How to Tell Them Apart
One of the most clinically important questions is: how do bowel obstruction symptoms differ from common conditions that cause similar discomfort?
Bowel Obstruction vs. Gastroenteritis (Stomach Bug)
Gastroenteritis typically causes nausea, vomiting, diarrhea, and cramping — but critically, there is usually active diarrhea. Bowel obstruction causes constipation and inability to pass gas. If someone is vomiting but also having diarrhea, obstruction is less likely (though a partial obstruction can sometimes cause paradoxical diarrhea). Additionally, gastroenteritis typically resolves within 24-72 hours, while obstruction symptoms progressively worsen.
Bowel Obstruction vs. Severe Constipation
Constipation causes discomfort and bloating, but typically without the severe colicky pain, significant vomiting, or high-pitched bowel sounds seen in obstruction. Laxatives or enemas may help with constipation; they are unlikely to resolve a true mechanical obstruction and may actually be harmful.
Bowel Obstruction vs. Irritable Bowel Syndrome (IBS)
IBS causes chronic abdominal pain with altered bowel habits, but it does not cause complete obstipation (inability to pass any gas or stool), severe vomiting, or fever. The pain of IBS typically responds to passing gas or having a bowel movement — bowel obstruction pain does not.
Bowel Obstruction vs. Appendicitis
Appendicitis causes pain that starts around the navel and moves to the right lower quadrant, combined with fever and nausea. Unlike bowel obstruction, it does not typically cause widespread abdominal distension or high-pitched bowel sounds early in the course.
Special Populations: How Symptoms May Present Differently
Elderly Patients
Older adults may present with more atypical symptoms. Pain may be less severe due to decreased pain sensitivity, fever may be absent even with serious infection, and the mental status change (confusion, delirium) may be the predominant presenting symptom. A high index of suspicion is needed in elderly patients with any change in bowel habits, abdominal discomfort, or unexplained confusion.
Children
Bowel obstruction in children often presents with intussusception (in infants) or adhesions from prior surgery (in older children). The classic presentation in infants is sudden episodes of severe crying that cause the infant to draw up their legs (indicating colicky pain), followed by periods of calm, along with vomiting and eventually "currant jelly" stools (dark, mucousy stools mixed with blood — a sign of bowel ischemia).
Patients with Prior Abdominal Surgery
Those who have had previous surgeries (especially bowel surgeries, hysterectomy, appendectomy) are at high risk for adhesion-related obstruction. They may develop obstructions years or even decades after their surgery with relatively sudden onset of symptoms.
What to Do When You Suspect Bowel Obstruction
If you recognize these symptoms — particularly the combination of abdominal pain, vomiting, distension, and inability to pass gas — here is what to do:
Do not eat or drink anything. Adding more to the system worsens the obstruction.
Do not take laxatives or enemas. These can increase pressure and potentially worsen or even perforate the bowel.
Do not apply heat to the abdomen. This does not help and may mask worsening symptoms.
Seek medical evaluation promptly — at an emergency room or by calling emergency services for severe symptoms.
Be prepared to describe your symptoms clearly: when they started, how they have changed, your last bowel movement and gas passage, any history of surgeries, and any current medications.
The Importance of Early Recognition
Bowel obstruction is a condition where time is genuinely critical. Every hour that passes with an untreated strangulation increases the likelihood of bowel necrosis, perforation, and the cascade of complications that follow. The difference between a short hospitalization with conservative management and an emergency surgery with bowel resection often comes down to how quickly the patient recognized the symptoms and sought care.
The symptoms described in this guide are your body's increasingly urgent signals that something is seriously wrong. Learning to read them — and acting on them — is one of the most valuable pieces of health knowledge you can have.