Colonic Diverticulosis: Understanding the Silent Condition in Your Colon
What Is Colonic Diverticulosis? A Comprehensive Overview
Colonic diverticulosis is one of the most prevalent yet most misunderstood gastrointestinal conditions in the modern world. It affects hundreds of millions of people globally, most of whom don't even know they have it. In fact, in many developed countries, colonic diverticulosis is considered an almost inevitable consequence of aging — a "wear and tear" condition of the large intestine that accumulates over decades of living on a low-fiber, Western-style diet. Yet despite its prevalence, diverticulosis rarely makes headlines, partly because the vast majority of those who have it never develop symptoms.
So what exactly is colonic diverticulosis, and why should you care about it? The answer lies in understanding the potential for this silent, asymptomatic condition to occasionally progress into something far more serious: diverticulitis, diverticular bleeding, or other complications that can dramatically affect quality of life. By understanding colonic diverticulosis thoroughly — what it is, why it develops, who is most at risk, and how it can be managed — you are empowered to take meaningful steps to protect your digestive health for years to come.

Defining Colonic Diverticulosis: The Anatomy Explained
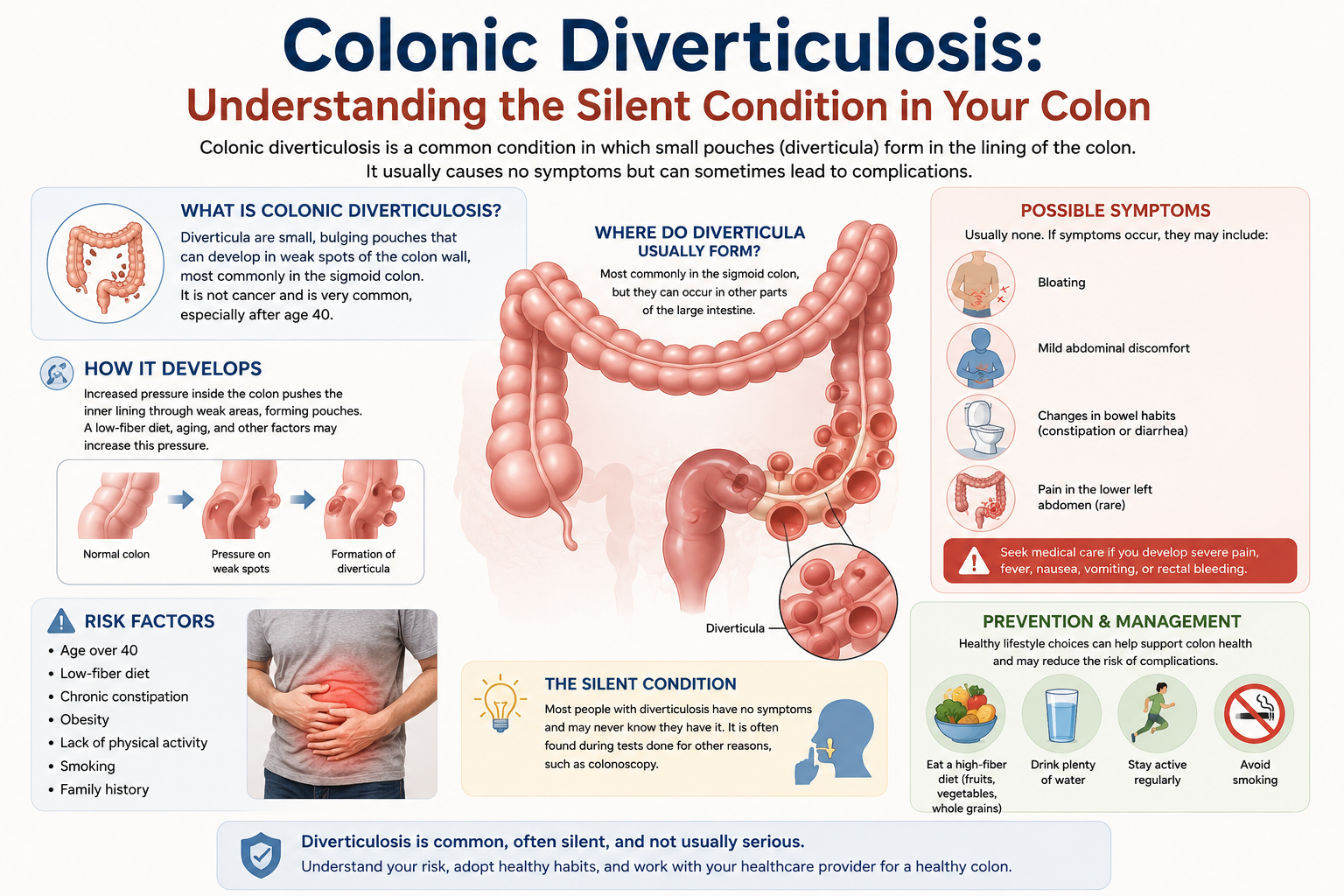
The word "diverticulosis" comes from the Latin "diverticulum," meaning a small pouch or sac. Colonic diverticulosis, therefore, refers specifically to the presence of these pouches in the colon (large intestine). To understand how these pouches form, it helps to know a little about colonic anatomy.
The colon, which is approximately 1.5 meters (5 feet) long in adults, is responsible for absorbing water and electrolytes from digestive residue and compacting waste into feces before elimination. The wall of the colon consists of several layers: the innermost mucosa (which includes absorptive cells), the submucosa (a supportive layer of connective tissue), two layers of smooth muscle (the inner circular and outer longitudinal), and the outermost serosa.
Diverticula form when the innermost mucosal and submucosal layers herniate (bulge outward) through weakened areas of the muscular wall. The most common sites of herniation are the areas where blood vessels (vasa recta) penetrate through the muscular layers — these natural gaps in the muscle create anatomical weak spots. The result is small, balloon-like pouches that protrude through the outer wall of the colon, typically measuring 5-10 mm in diameter, though they can occasionally reach several centimeters.
There are two anatomical types of diverticula: true diverticula and false diverticula (pseudodiverticula). True diverticula involve all layers of the bowel wall, while the far more common false diverticula (which are what we typically see in colonic diverticulosis) involve only the mucosal and submucosal layers pushing through the muscular wall. The colonic diverticula seen in diverticulosis are almost always of the false type.
Geographically, diverticulosis predominantly affects the sigmoid colon (the S-shaped segment of the colon on the lower left side of the abdomen) in Western populations. This is thought to be related to the fact that the sigmoid colon is the narrowest part of the colon and experiences the highest intraluminal pressures during bowel movements. In contrast, studies from Asia (particularly Japan, Korea, and China) have historically found that right-sided colonic diverticulosis (affecting the cecum and ascending colon) is more common, though this pattern is changing as Asian populations adopt more Westernized diets.
Epidemiology: How Common Is Colonic Diverticulosis?
The prevalence of colonic diverticulosis is strongly correlated with age and geography. In Western nations, prevalence data from autopsy series and colonoscopy studies reveal a clear age-dependent pattern: approximately 10-25% of adults under age 50 have diverticulosis, while the prevalence rises to over 50% in those aged 60-70 and approaches 65-70% in individuals over the age of 80. Some studies suggest even higher figures, with certain populations showing diverticulosis in more than 80% of individuals over 85.
In terms of absolute numbers, diverticular disease (which includes both diverticulosis and diverticulitis) accounts for more than 313,000 hospitalizations and 1.5 million outpatient visits in the United States annually. The economic burden of diverticular disease in the U.S. alone is estimated at over $2.4 billion per year in direct medical costs.
Globally, rates of diverticulosis are substantially lower in sub-Saharan Africa, rural Asia, and other regions where high-fiber diets are the norm. This striking geographic variation was first noted by the British physician Denis Burkitt in the 1970s, leading to the "dietary fiber hypothesis," which posited that low dietary fiber intake was the primary driver of diverticulosis development. While subsequent research has nuanced this hypothesis considerably, dietary fiber remains one of the most important modifiable risk factors for the condition.
The Root Causes of Colonic Diverticulosis
The development of colonic diverticulosis is multifactorial, meaning it results from the interplay of multiple factors including diet, gut motility, intestinal structure, gut microbiome composition, genetics, and aging. Understanding these causes helps explain both why diverticulosis is so common in Western populations and what can be done to prevent it.
Dietary Fiber Deficiency
The relationship between low dietary fiber intake and colonic diverticulosis has been extensively studied since Burkitt's pioneering observations. Dietary fiber increases stool bulk and softens stool consistency, reducing the force of muscular contractions needed to propel stool through the colon. When dietary fiber is insufficient, stools become hard and small, requiring high-pressure segmental contractions to move them along. This increased intraluminal pressure is transmitted to the colon wall, which over years and decades of repetitive stress causes weakening and eventual herniation of the mucosal layer at vulnerable points.
Multiple large cohort studies have confirmed the inverse relationship between fiber intake and diverticular disease risk. The Health Professionals Follow-Up Study, which followed over 47,000 male health professionals for years, found that those with the highest fiber intake had a significantly lower risk of symptomatic diverticular disease compared to those with the lowest intake.
Alterations in Gut Motility and Colonic Pressure
Modern understanding of diverticulosis pathogenesis extends well beyond simple fiber deficiency. Research has shown that abnormalities in colonic motility — the rhythmic muscular contractions that propel intestinal contents — play an important role. In patients with diverticulosis, studies using colonoscopy and manometry (pressure measurements) have found higher baseline colonic pressures and more intense segmental contractions compared to healthy controls, even after controlling for dietary factors.
These motility abnormalities may be related to changes in the enteric nervous system (the "second brain" of the gut), alterations in gut hormones, reduced smooth muscle compliance with aging, or changes in the gut microbiome that affect neurotransmitter production and motility regulation.
Aging and Structural Changes in the Colon Wall
Age-related changes in the colon wall are a fundamental contributor to diverticulosis risk. As we age, the collagen matrix of the connective tissue layers becomes stiffer and less elastic. Studies using electron microscopy have shown that colonic connective tissue in older individuals has higher collagen crosslinking, which paradoxically makes the tissue both stiffer (more resistant to stretching) and more fragile (more prone to rupturing under repeated stress). These structural changes increase vulnerability to herniation at points of anatomical weakness.
Interestingly, connective tissue disorders such as Marfan syndrome, Ehlers-Danlos syndrome, and scleroderma are associated with significantly higher rates of diverticulosis at younger ages, further supporting the role of connective tissue integrity in diverticulosis pathogenesis.
Physical Inactivity and Obesity
Sedentary lifestyle has been consistently identified as a risk factor for diverticulosis and its complications. Regular physical activity promotes gut motility, reduces constipation, decreases intracolonic pressure, and may modulate the gut microbiome in ways that are protective. Several prospective studies have found that men who exercised vigorously had significantly lower rates of diverticular disease compared to their sedentary counterparts.
Obesity — particularly visceral (abdominal) adiposity — is associated with chronic low-grade inflammation, alterations in gut microbiome composition, and potentially increased intraabdominal pressure, all of which may contribute to diverticulosis development and the risk of progression to diverticulitis.
Genetic Factors
A genetic component to diverticular disease has been suggested by family and twin studies. A large Swedish twin study found that genetic factors accounted for approximately 40% of the variance in diverticular disease susceptibility, suggesting a substantial heritable component. Specific genetic polymorphisms affecting connective tissue metabolism, immune function, and gut motility have been proposed as contributors, though no specific "diverticulosis gene" has been definitively identified.
Gut Microbiome Dysbiosis
An emerging area of research concerns the role of the gut microbiome — the community of trillions of bacteria, viruses, and fungi inhabiting the colon — in diverticulosis development and progression. Studies have found differences in microbiome composition between individuals with and without diverticular disease, with some suggesting that dysbiosis (imbalance in microbial communities) contributes to abnormal motility, low-grade inflammation, and increased mucosal permeability. While the evidence remains preliminary, the gut microbiome is increasingly viewed as a potential therapeutic target.

Symptoms of Colonic Diverticulosis: The Silent Majority
One of the most important clinical facts about colonic diverticulosis is that the vast majority of affected individuals — approximately 70-80% — are completely asymptomatic. They have diverticula scattered throughout their colon, but these pouches cause no pain, no change in bowel habits, and no other symptoms. In these individuals, diverticulosis is discovered incidentally during colonoscopy performed for cancer screening, during CT imaging for another indication, or at autopsy.
However, a subset of patients with diverticulosis do report symptoms. These symptoms are collectively referred to as "symptomatic uncomplicated diverticular disease" (SUDD) or, in older literature, "painful diverticular disease." Symptoms of SUDD can include:
Chronic, intermittent lower abdominal pain: Usually located in the left lower quadrant (overlying the sigmoid colon), this pain tends to be cramping or dull in character, may worsen after eating, and often improves with bowel movements or passing gas.
Bloating and flatulence: Many patients with diverticulosis report a persistent sensation of abdominal fullness and excessive gas production.
Altered bowel habits: Some patients experience constipation, diarrhea, or alternating constipation and diarrhea, which may be difficult to distinguish from irritable bowel syndrome (IBS).
A sensation of incomplete evacuation: A feeling that the bowel hasn't fully emptied after a bowel movement.
It's worth noting that the relationship between diverticulosis and these symptoms is not entirely straightforward. Research has suggested that many of the symptoms attributed to "symptomatic diverticulosis" may in fact be due to co-existing IBS, microscopic colitis, or other functional gastrointestinal disorders rather than the diverticula themselves. This diagnostic ambiguity has important treatment implications.
Complications of Colonic Diverticulosis
While most people with diverticulosis live their entire lives without ever experiencing a significant complication, a meaningful minority (approximately 20-25% of those with diverticulosis) will develop at least one complication during their lifetime. The two principal complications are diverticulitis and diverticular bleeding.
Diverticulitis
Diverticulitis occurs when one or more diverticula become inflamed or infected. The exact mechanism by which this occurs is not fully understood, but it is believed to involve either micro-perforation (a tiny hole in the diverticulum wall allowing bacteria to escape into the pericolic fat) or obstruction of the diverticulum opening by hardened fecal material (a fecalith), leading to bacterial overgrowth and mucosal injury. Diverticulitis can range from mild (uncomplicated) to severe (complicated, with abscess, perforation, or fistula formation).
Diverticular Bleeding
Diverticular bleeding is the most common cause of major lower gastrointestinal bleeding in adults, accounting for approximately 30-40% of all lower GI bleeding episodes. It occurs when one of the blood vessels (vasa recta) that runs along the dome of a diverticulum erodes or ruptures, causing bright red blood per rectum. Diverticular bleeding is often painless and can be dramatic in volume, sometimes requiring hospitalization and transfusion. Fortunately, 70-80% of episodes stop spontaneously, though the risk of rebleeding is significant.
How Is Colonic Diverticulosis Diagnosed?
As mentioned above, colonic diverticulosis is most often diagnosed incidentally during procedures or tests performed for other reasons. The most common diagnostic modalities include:
Colonoscopy
Colonoscopy — the gold standard examination of the colon — allows direct visualization of the colon's interior, including the mouths of diverticula. The endoscopist can see the diverticula as small openings or craters along the colonic wall. Colonoscopy is also important for ruling out other conditions (such as colorectal polyps or cancer) that may cause similar symptoms, and it should be performed in all patients with unexplained lower GI bleeding once an acute bleed has been controlled.
CT Colonography (Virtual Colonoscopy)
CT colonography uses computed tomography imaging to create a detailed 3D map of the colon. It can identify diverticula and assess for other colonic pathology without requiring endoscopy. It is less sensitive than traditional colonoscopy for detecting small polyps but is a reasonable alternative for patients who cannot or will not undergo colonoscopy.
CT Scan of the Abdomen and Pelvis
During a CT scan performed for abdominal pain or other indications, diverticula may be clearly visible as outpouchings along the colonic wall. CT is the primary modality used to diagnose and grade diverticulitis when it develops.
Barium Enema
Barium enema — an older radiological technique in which barium contrast is instilled into the colon through the rectum and X-rays are taken — can clearly demonstrate multiple diverticula as small barium-filled pouches projecting from the colon wall. While largely supplanted by colonoscopy and CT in modern practice, it remains occasionally used in certain settings.
Distinguishing Colonic Diverticulosis from Other Conditions
Because colonic diverticulosis shares some symptoms (particularly lower abdominal pain and altered bowel habits) with other gastrointestinal conditions, it's important for clinicians to consider a broad differential diagnosis. Key conditions to distinguish from symptomatic diverticulosis include:
Irritable Bowel Syndrome (IBS): IBS is a functional bowel disorder characterized by recurrent abdominal pain, bloating, and changes in bowel habits, without organic pathology. The overlap in symptoms between IBS and symptomatic diverticulosis is significant, and many patients have both conditions simultaneously. Differentiating them is important because treatments differ.
Colorectal Cancer: Both colorectal cancer and diverticulosis can cause abdominal pain, change in bowel habits, and rectal bleeding. Because colorectal cancer is potentially life-threatening, it must always be ruled out — particularly in patients over 50 with new symptoms.
Inflammatory Bowel Disease (IBD): Crohn's disease and ulcerative colitis can also cause abdominal pain, diarrhea, and rectal bleeding. Colonoscopy with biopsy and imaging are important for distinguishing IBD from diverticular disease.
Ischemic Colitis: Reduced blood flow to the colon can cause abdominal cramping and bloody diarrhea that may mimic diverticular disease. CT scan with IV contrast can help identify characteristic patterns of ischemic colitis.
Ovarian and Gynecological Conditions: In women, ovarian cysts, endometriosis, and pelvic inflammatory disease can cause left lower quadrant pain that may be confused with sigmoid diverticular symptoms.
Management of Colonic Diverticulosis: What Does the Evidence Say?
The management of asymptomatic colonic diverticulosis focuses primarily on lifestyle modifications aimed at preventing the development of diverticulitis or diverticular bleeding. For symptomatic diverticulosis (SUDD), treatment aims to reduce symptoms while also preventing complications.
High-Fiber Diet
Increasing dietary fiber intake is the cornerstone recommendation for patients with colonic diverticulosis. Current guidelines recommend 25-35 grams of fiber per day for adults, significantly more than the average American currently consumes (approximately 15-18 grams per day). The benefits of a high-fiber diet include softer, bulkier stools that are easier to pass, reduced intracolonic pressure, and potentially modulation of the gut microbiome in ways that reduce inflammation.
Fiber can be obtained from a variety of food sources: fruits (particularly those with edible skins and seeds), vegetables, legumes (lentils, beans, chickpeas), whole grains (oats, barley, brown rice, whole wheat), and nuts and seeds. Fiber supplements containing psyllium husk, methylcellulose, or inulin can also be used to supplement dietary intake, though food sources are generally preferred for their additional nutritional benefits.
An important note: for many years, physicians advised patients with diverticulosis to avoid eating nuts, seeds, corn, and popcorn out of concern that these small particles could become lodged in diverticula and trigger diverticulitis. However, a large prospective study published in JAMA in 2008 (Strate et al.) found no increased risk of diverticulitis or diverticular bleeding associated with consumption of these foods. Current guidelines no longer recommend avoiding nuts, seeds, popcorn, or corn in patients with diverticulosis.
Physical Activity
Regular physical exercise promotes gut motility, reduces constipation, and may reduce the risk of complications. Current recommendations suggest at least 150 minutes of moderate-intensity aerobic activity per week, though more vigorous exercise appears to offer additional protection against diverticular complications based on epidemiological data.
Weight Management
Maintaining a healthy body weight through a combination of diet and exercise reduces multiple risk factors simultaneously: systemic inflammation, constipation, gut motility problems, and potentially microbiome dysbiosis.
Adequate Hydration
Drinking sufficient water (typically 6-8 glasses per day) is essential to allow dietary fiber to function properly. Fiber without adequate water can paradoxically worsen constipation by making stool firmer and harder to pass.
Mesalazine and Rifaximin for Symptomatic Diverticulosis
For patients with symptomatic uncomplicated diverticular disease (SUDD), medications may be considered. Rifaximin — a poorly absorbed oral antibiotic — has been studied in combination with fiber supplementation and shown in several randomized controlled trials (particularly European ones) to reduce symptoms of SUDD compared to fiber alone. The proposed mechanism involves reduction of gut bacterial overgrowth and associated inflammation. Mesalazine (5-aminosalicylic acid), an anti-inflammatory medication used in IBD, has also been studied in diverticulosis with mixed results; some trials suggest modest symptom benefit, while others show no significant advantage over placebo.
Probiotics
Given the emerging evidence for gut microbiome involvement in diverticular disease, probiotics have been investigated as a potential therapeutic tool. Some small studies have suggested that certain probiotic strains may reduce symptoms of SUDD, but the evidence base is not yet sufficient to make firm recommendations. Probiotics are generally safe and may offer some benefit as an adjunct to dietary and lifestyle measures.

Monitoring and Follow-Up for Colonic Diverticulosis
Because the natural history of diverticulosis is generally benign for most patients, there are no established guidelines requiring regular colonoscopic surveillance specifically for diverticulosis (unlike colorectal polyps, which do require surveillance). However, it is important for patients with diverticulosis to:
Maintain regular check-ups with their primary care physician or gastroenterologist, particularly if they develop new or worsening symptoms. Be aware of the warning signs of diverticulitis (left lower quadrant pain, fever, nausea) and seek medical attention promptly if these occur. Undergo colonoscopy or other colon evaluation after any episode of diverticulitis or significant diverticular bleeding to rule out underlying colorectal malignancy and to fully assess the extent of diverticular disease. Adhere to recommended colorectal cancer screening guidelines, independent of their diverticulosis diagnosis.
Living With Colonic Diverticulosis: A Patient's Perspective
Receiving a diagnosis of colonic diverticulosis can be alarming for patients, particularly because the word "disease" implies something serious. However, it's important to understand that for most people, diverticulosis is a manageable chronic condition that need not significantly impair quality of life. The vast majority of affected individuals will never develop diverticulitis or diverticular bleeding. Those who do experience complications have a good prognosis with appropriate treatment.
The key to living well with diverticulosis is adopting a proactive approach to digestive health: eating a diet rich in fiber from diverse plant sources, staying physically active, maintaining a healthy weight, drinking adequate water, and keeping your healthcare provider informed of any new or changing symptoms. These relatively simple lifestyle adjustments can significantly reduce your risk of complications and contribute to better overall health in numerous ways beyond digestive function.
For those who do experience symptoms — the SUDD population — working closely with a gastroenterologist to find the right combination of dietary, lifestyle, and potentially pharmacological interventions is essential. It may take time and some trial and error to find what works best for your individual situation, but with patience and persistence, most patients can achieve good symptom control.
The Future of Colonic Diverticulosis Research
As the global prevalence of diverticulosis continues to rise — driven by aging populations, dietary changes in emerging economies, and possibly increasing use of medications such as NSAIDs and opioids — research into this condition is intensifying. Several exciting areas of investigation are underway:
Microbiome research is exploring whether specific microbial signatures can predict which patients with diverticulosis are most likely to develop diverticulitis, potentially enabling personalized prevention strategies. Genetic studies are working to identify specific genetic variants that confer risk or protection, which could eventually lead to targeted therapies. Novel anti-inflammatory agents and gut motility modulators are being developed and tested for prevention of diverticular complications. Minimally invasive surgical techniques continue to advance, improving outcomes for patients who do require surgical intervention.
Conclusion
Colonic diverticulosis is a remarkably common condition — affecting the majority of older adults in Western countries — that is often silent, discovered incidentally, and benign in most cases. Yet it is also the precursor to potentially serious complications including diverticulitis and diverticular bleeding that together impose a significant burden of illness and healthcare costs. Understanding the biology, risk factors, natural history, and management of colonic diverticulosis empowers patients and clinicians alike to make better-informed decisions about prevention, monitoring, and treatment.
If you have been diagnosed with colonic diverticulosis — or if you have risk factors such as older age, a low-fiber diet, physical inactivity, or family history — the most important thing you can do is take actionable steps now to reduce your risk of complications. Embrace a high-fiber diet, move your body regularly, stay hydrated, and maintain open communication with your healthcare team. Your colon is a remarkable organ that plays a vital role in your health; taking care of it will pay dividends for years to come.