Diverticulitis Symptoms in Females: A Gender-Specific Complete Guide
Diverticulitis in Women: Understanding the Female Experience
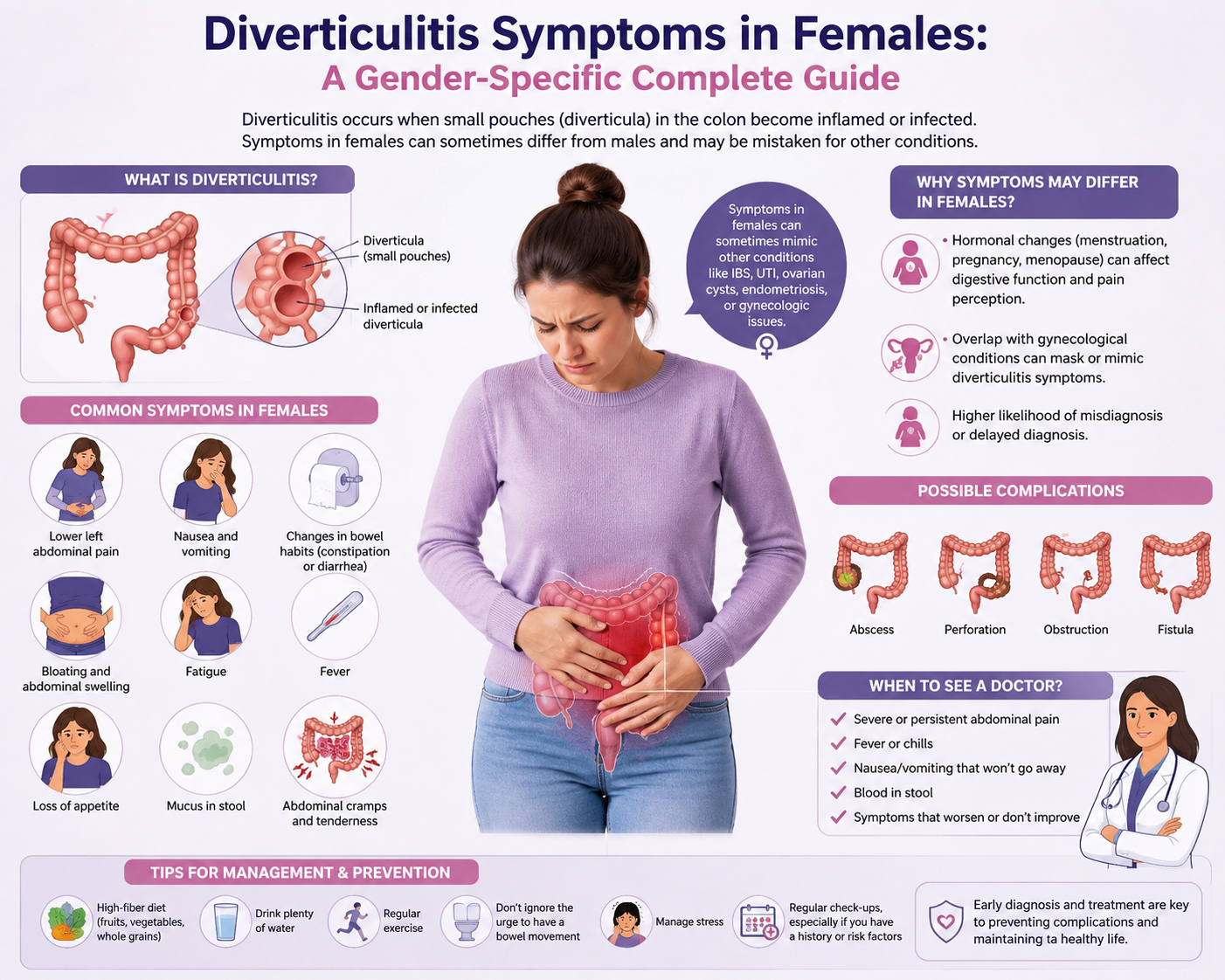
Diverticulitis affects both men and women, but the experience of this condition can differ significantly between the sexes. Women face a unique set of diagnostic challenges, symptom presentations, and biological influences — including hormonal factors, pelvic anatomy, and gynecological conditions that can mimic or coexist with diverticulitis — that make accurate diagnosis and appropriate management more complex. This comprehensive guide focuses specifically on diverticulitis symptoms in females, examining how women experience this condition differently from men, what the research tells us about gender-specific aspects of the disease, and how women can best advocate for themselves when navigating the healthcare system with a potential diverticulitis diagnosis.
Epidemiology: How Diverticulitis Affects Women Differently from Men
The relationship between diverticular disease and sex is nuanced and has evolved in our understanding over recent decades. Historically, diverticulitis was considered more common in men under the age of 50 and more common in women over 50, a pattern thought to reflect hormonal influences. Research from large population-based studies in more recent years has continued to show that while diverticulosis (the presence of diverticula) affects men and women at broadly similar rates overall, the risk of progression from diverticulosis to diverticulitis and the severity of disease appear to differ by sex.
Among younger adults (under 50), diverticulitis is more common in men. However, after menopause, women's risk increases substantially — and some studies show that postmenopausal women have a higher overall risk of complicated diverticulitis than age-matched men. This shift in risk across the menopausal transition has led researchers to investigate the potential role of estrogen in modulating gut inflammation and colon motility, though the mechanisms remain incompletely understood.
Women with diverticulitis also appear to be at higher risk for complicated disease at first presentation. Several retrospective studies have found that women are more likely than men to present with complicated diverticulitis (abscess, perforation, or fistula) at initial diagnosis, possibly because their symptoms are more difficult to distinguish from gynecological conditions, leading to diagnostic delays.

Classic Diverticulitis Symptoms in Women
The core symptoms of diverticulitis in women are broadly similar to those in men, though their location and character can sometimes be confused with other conditions. Understanding these classic symptoms is the first step toward seeking appropriate care promptly.
Lower Abdominal Pain
Abdominal pain is the hallmark symptom of diverticulitis in both sexes, and in women as in men, it most commonly affects the lower-left quadrant of the abdomen (overlying the sigmoid colon). This pain is typically described as a constant, dull ache or cramping sensation that may range from mild (barely noticeable) to severe (incapacitating). The pain often develops gradually over a period of days, though in some cases it can come on more suddenly.
However, women face a particular challenge: the lower left abdomen is also the region of the left ovary and fallopian tube, as well as part of the uterus. Left lower quadrant pain in women therefore has a significantly broader differential diagnosis than in men, encompassing ovarian cysts, ovarian torsion, ectopic pregnancy, endometriosis, pelvic inflammatory disease (PID), and uterine conditions, in addition to diverticulitis and other gastrointestinal causes. This overlap creates diagnostic ambiguity that can result in delayed or incorrect initial diagnoses.
Fever
Fever — typically a low-grade temperature of 100.4-102°F (38-39°C) — is a common feature of acute diverticulitis reflecting the body's inflammatory response to infection. In women, fever associated with lower abdominal pain may prompt immediate investigation for pelvic inflammatory disease (PID) or tubo-ovarian abscess, which are also infectious conditions affecting the reproductive organs. The coexistence of fever and lower abdominal pain should always prompt comprehensive evaluation to distinguish between gastrointestinal and gynecological causes.
Nausea and Vomiting
Many women with diverticulitis experience nausea, and some vomit. These symptoms reflect the effect of inflammatory cytokines on gut motility and the overall physiological stress of an acute inflammatory episode. In some women, nausea and vomiting may be the predominant presenting symptoms rather than pain, which can further complicate the diagnostic picture.
Changes in Bowel Habits
Diverticulitis commonly causes alterations in bowel habits. In women, this most often manifests as constipation, though diarrhea can also occur, as can alternating constipation and diarrhea. Urgent bowel movements, increased frequency, or a sensation of incomplete evacuation may also be reported. These bowel changes may be accompanied by mucus in the stool.
Bloating and Abdominal Distension
Abdominal bloating and distension — a feeling of fullness and visible swelling of the abdomen — are commonly reported by women with diverticulitis. This symptom reflects the inflammatory process in the colon and the associated disruption of normal gut motility. Women are generally more prone to bloating-related symptoms than men across a range of gastrointestinal conditions, which may reflect differences in gut sensitivity and hormone-mediated motility changes.
Gender-Specific Symptoms and Complications in Women
Beyond the classic diverticulitis symptoms described above, women experience certain aspects of diverticulitis that are either unique to or more common in the female population due to their anatomy and physiology.
Colovaginal Fistula: A Female-Specific Complication
One of the most significant female-specific complications of diverticulitis is the colovaginal fistula — an abnormal connection that develops between the inflamed, perforated segment of the colon and the vagina. This complication is the result of chronic, unresolved diverticular inflammation eroding through the wall of the adjacent vagina.
The symptoms of a colovaginal fistula are distinctive and alarming: passage of gas (flatus) from the vagina, passage of fecal material from the vagina (fecaluria), and persistent vaginal discharge that may have a feculent odor. These symptoms are unmistakable and virtually diagnostic when they occur, though they are understandably distressing and sometimes embarrassing for affected women, which may delay help-seeking.
Colovaginal fistulas are significantly more common in women than colovesical fistulas (colon-to-bladder fistulas, which occur predominantly in men, because the male bladder sits lower and closer to the sigmoid colon in men than in women, where the uterus acts as an anatomical barrier between the sigmoid colon and the bladder). The management of colovaginal fistulas typically requires surgical intervention — usually elective sigmoid colectomy with primary anastomosis and repair of the vaginal defect.
Interaction with Endometriosis
Endometriosis — a condition in which endometrial-like tissue grows outside the uterus — affects approximately 10% of women of reproductive age and can cause significant chronic lower abdominal and pelvic pain. The pain of endometriosis, particularly when it affects the sigmoid colon (intestinal endometriosis), can closely mimic diverticulitis, including causing lower left quadrant pain, bloating, altered bowel habits, and pain with defecation (dyschezia).
More importantly, both conditions can coexist in the same patient, making the diagnostic challenge even greater. A woman with known endometriosis who develops new or worsening lower abdominal pain may reasonably assume it is an endometriosis flare, potentially delaying investigation for diverticulitis. Clinicians managing women with known endometriosis must maintain a low threshold for considering diverticulitis in the differential diagnosis, particularly in older patients.
Ovarian Cyst and Diverticulitis: The Diagnostic Dilemma
Ovarian cysts — fluid-filled sacs on the ovary — are extremely common in women of reproductive age and are usually asymptomatic. However, when an ovarian cyst ruptures or becomes large, it can cause sudden, severe left lower quadrant pain, with or without fever and nausea, creating a presentation virtually indistinguishable from acute diverticulitis without imaging.
The distinction is critically important because the management is completely different: ruptured or hemorrhagic ovarian cysts may require gynecological intervention, while diverticulitis requires antibiotics and possibly gastroenterological or surgical management. CT scan of the abdomen and pelvis with contrast is typically the most reliable imaging modality for distinguishing between these conditions in the acute setting, though transvaginal ultrasound can also be helpful for assessing the adnexa (ovaries and tubes).
Menstrual Cycle Influences on Symptom Severity
Some women with chronic symptomatic diverticular disease or recurrent diverticulitis report that their symptoms are influenced by the menstrual cycle. Premenstrual and menstrual symptom exacerbations of abdominal pain, bloating, and altered bowel habits are common in the general female population (partly due to prostaglandin-mediated smooth muscle effects), and these hormone-related symptom fluctuations can make it difficult to distinguish between menstrual pain and diverticular pain flares.
Estrogen and progesterone have well-documented effects on gut motility. Progesterone — which is elevated in the luteal phase of the menstrual cycle and throughout pregnancy — slows gut motility and may worsen constipation. This progesterone-driven constipation during the luteal phase may theoretically increase intraluminal pressure and the risk of triggering a diverticulitis episode in susceptible women. However, prospective evidence specifically linking menstrual phase to diverticulitis flare risk is limited.

Hormonal Influences: The Role of Estrogen in Diverticular Disease
The observation that diverticulitis risk in women increases substantially after menopause has fueled interest in the potential protective role of estrogen against diverticular inflammation. Several biological mechanisms could explain an estrogen-protective effect:
Gut motility regulation: Estrogen promotes intestinal motility, helping to prevent constipation. Postmenopausal women with low estrogen levels may experience worsened gut motility, increased transit time, and greater intracolonic pressure — all of which promote diverticular disease.
Immune modulation: Estrogen has known immunomodulatory properties and promotes anti-inflammatory immune responses. Loss of estrogen at menopause may shift the immune environment of the gut mucosa toward a more pro-inflammatory state.
Gut microbiome modulation: Estrogen receptors are present in the gut, and estrogen influences gut microbiome composition. Postmenopausal estrogen deficiency has been associated with changes in the gut microbiome toward less diverse and potentially more dysbiotic communities.
Collagen synthesis: Estrogen supports collagen synthesis and connective tissue integrity. Estrogen deficiency after menopause accelerates age-related collagen degradation, potentially increasing colonic wall vulnerability to diverticula formation.
Studies examining hormone replacement therapy (HRT) and diverticular disease risk have produced somewhat mixed results, with some observational studies suggesting a modest protective effect of HRT on diverticulitis risk, while others have shown no significant association. Given the complexity of HRT effects on the body and the multiple confounders in observational studies, no definitive recommendations about HRT for diverticulitis prevention can be made at this time.
Diagnostic Challenges Specific to Women
The breadth of conditions that can mimic diverticulitis in women creates significant diagnostic challenges that can lead to delays in appropriate treatment. Understanding these challenges helps women advocate for themselves and helps clinicians provide better care.
The Broad Differential Diagnosis
When a woman presents with lower left abdominal pain, fever, and nausea, the differential diagnosis includes not only diverticulitis but also: ovarian cyst (simple, hemorrhagic, or ruptured); ovarian torsion (twisting of the ovary); ectopic pregnancy (a medical emergency requiring immediate exclusion in women of reproductive age); pelvic inflammatory disease (PID); tubo-ovarian abscess; endometriosis flare; uterine fibroids with degeneration; appendicitis (particularly when the appendix is in an atypical location); urinary tract infection or pyelonephritis; and irritable bowel syndrome.
This extensive differential means that women with diverticulitis are more likely than men to undergo additional diagnostic tests, including pelvic ultrasound and gynecological examination, before the correct diagnosis of diverticulitis is made.
The Importance of CT Scan
For women with acute lower abdominal pain of uncertain cause, CT scan of the abdomen and pelvis with intravenous contrast remains the most valuable single imaging study for sorting through this complex differential diagnosis. CT can simultaneously evaluate the colon (for diverticulitis), the ovaries (for cysts or torsion), the uterus, the appendix, and the urinary tract in a single examination. While MRI avoids radiation exposure and may be preferred in pregnant patients, CT is typically faster, more widely available, and provides excellent detail for acute abdominal evaluation.
Transvaginal ultrasound (TVUS) is an excellent first-line imaging tool for evaluating the uterus and adnexa (ovaries and tubes) but has limited ability to visualize the colon. Therefore, TVUS and CT are often complementary rather than interchangeable, and both may be needed in women with complex presentations.
The Risk of Diagnostic Delay in Women
Multiple retrospective studies have found that women with diverticulitis wait longer on average to receive a definitive diagnosis compared to men, largely because of the broader differential diagnosis requiring exclusion of gynecological conditions. This diagnostic delay has clinical consequences: women are more likely to present with complicated diverticulitis (abscess, perforation) at first diagnosis, and they undergo more diagnostic procedures, including laparoscopy, before the correct diagnosis is established.
Women should feel empowered to advocate for themselves during the diagnostic process. If you are experiencing lower abdominal pain, fever, and nausea, it is entirely appropriate to ask your physician specifically about diverticulitis as a possible diagnosis — even if you are also being evaluated for gynecological conditions. Both evaluations can and should proceed simultaneously.
Treatment of Diverticulitis in Women: Are There Gender-Specific Considerations?
The fundamental principles of diverticulitis treatment are the same for men and women: dietary modification during acute episodes, antibiotics for moderate to severe or complicated cases, and supportive care. However, several treatment considerations are specific to or particularly important for women.
Pregnancy and Diverticulitis
Diverticulitis during pregnancy is rare but represents a particularly challenging clinical situation. The gravid uterus displaces the colon, potentially changing the location and character of pain. Constipation — a common symptom of pregnancy related to hormonal changes (particularly progesterone's effect on gut motility) and the pressure of the growing uterus — may predispose pregnant women to diverticulitis episodes. Diagnosis is challenging because CT imaging (the gold standard) requires judicious use in pregnancy due to radiation exposure; MRI is preferred when available, though it is more expensive and time-consuming. Treatment typically follows standard principles with appropriate antibiotic selection (avoiding antibiotics teratogenic to the fetus) and careful monitoring. Surgical intervention, if required, is associated with higher maternal and fetal complication rates and should be performed at centers with experience in obstetric surgery.
Antibiotic Selection
Standard antibiotic regimens for diverticulitis (fluoroquinolones, metronidazole, amoxicillin-clavulanate) are generally appropriate for both sexes. However, in women of childbearing age, the potential for pregnancy must be considered before prescribing fluoroquinolones (generally avoided in pregnancy) or metronidazole (used cautiously in the first trimester). A pregnancy test should be performed in women of reproductive age presenting with acute abdominal pain before initiating antibiotic therapy for presumed diverticulitis.
Surgical Decision-Making
The decision about elective sigmoid colectomy (surgery to prevent future episodes) in women with recurrent diverticulitis involves considerations specific to female anatomy. For women of reproductive age, surgeons must consider the potential impact of sigmoid colectomy on fertility and on future pregnancies, as adhesion formation following pelvic surgery can affect fertility. Minimally invasive (laparoscopic) surgery reduces adhesion formation compared to open surgery and is generally preferred in women who may wish to conceive. Women who are postmenopausal or who have completed their families have fewer of these concerns, and surgical decision-making is more similar to that in men.
Prevention and Long-Term Management for Women
The evidence-based prevention strategies for diverticulitis in women are essentially the same as for the general population, with a few considerations particularly relevant to women:
High-fiber diet: Increasing dietary fiber to 25-35g/day is the foundational recommendation. Women on average consume less dietary fiber than men in most Western countries, making this particularly important as a preventive measure.
Regular physical activity: Exercise is consistently protective against diverticulitis. Beyond its specific gut benefits, exercise is also beneficial for women's hormonal health, bone density, cardiovascular risk, and overall wellbeing.
Weight management: Maintaining a healthy BMI reduces systemic inflammation and improves gut motility. Postmenopausal women may face particular challenges with weight management due to hormonal changes, making dietary attention and regular physical activity especially important during this life stage.
NSAID use: Women who use NSAIDs regularly for conditions such as dysmenorrhea (painful periods), arthritis, or headaches should discuss the implications of regular NSAID use with their physicians in the context of diverticular disease. Acetaminophen is generally a preferable analgesic for women with diverticular disease when adequate pain relief can be achieved.
Probiotic supplementation: While the evidence base for probiotics in diverticular disease prevention remains preliminary, probiotics are generally safe and well-tolerated. Some evidence suggests they may help maintain microbiome diversity and reduce low-grade gut inflammation — potential benefits that are equally relevant for women and men.
When Should Women Seek Emergency Care?
Certain symptoms in women with suspected or known diverticulitis require immediate emergency medical attention:
Sudden, severe lower abdominal pain (particularly if it comes on very suddenly and is the "worst pain of your life" — this raises concern for ovarian torsion, ruptured ectopic pregnancy, or perforated diverticulitis); positive pregnancy test combined with lower abdominal pain and/or vaginal bleeding (ectopic pregnancy must be immediately excluded); high fever above 102°F (39°C) combined with severe abdominal pain; any signs of hemodynamic instability (lightheadedness, fainting, rapid heart rate, confusion); symptoms of peritonitis including board-like abdominal rigidity and inability to move without severe pain; passage of gas or fecal material from the vagina (suggesting colovaginal fistula).
Frequently Asked Questions from Women About Diverticulitis
Can diverticulitis be confused with ovarian cysts?
Yes, absolutely. Both conditions can cause left lower quadrant abdominal pain, often with similar character and severity. CT scan of the abdomen and pelvis is typically necessary to distinguish between them with confidence. Pelvic ultrasound can help evaluate the ovaries but cannot reliably assess the colon, so it usually needs to be combined with CT imaging in the acute setting.
Is diverticulitis worse after menopause?
Research suggests that postmenopausal women face a higher risk of diverticulitis compared to premenopausal women. Whether this reflects reduced estrogen's protective effects on the gut, age-related changes in the colon, or other factors is not fully established. Maintaining the protective lifestyle factors (high fiber diet, regular exercise, healthy weight) is particularly important for postmenopausal women.
Can diverticulitis affect my ability to get pregnant?
Uncomplicated diverticulitis in a woman of reproductive age does not directly affect fertility. However, complicated diverticulitis requiring surgery (particularly emergency Hartmann's procedure or any open pelvic surgery) can result in adhesion formation that affects the fallopian tubes and ovaries, potentially impairing fertility. For this reason, minimally invasive surgical approaches are preferred in women who have not completed their families.
Conclusion
Diverticulitis in women presents a uniquely complex clinical picture. The overlap with gynecological conditions makes diagnosis more challenging, hormonal factors influence disease risk and progression, and female-specific complications such as colovaginal fistula require specialized management. Women dealing with unexplained lower abdominal pain — particularly those over 40 — should be aware of diverticulitis as a potential cause, especially if they have known risk factors for diverticular disease. Early and accurate diagnosis, appropriate treatment, and commitment to evidence-based prevention strategies are the keys to managing diverticulitis effectively and minimizing its impact on quality of life. Working with a team that includes both a gastroenterologist and a gynecologist is often the optimal approach for women with complex presentations or recurrent disease.