Female Pancreatitis Pain Location: Where It Hurts and Why It's Different
Introduction: Why Gender Matters in Pancreatitis
When most people think about pancreatitis, they picture a single, universal experience: sudden, severe pain in the upper abdomen that radiates to the back. While this description is medically accurate as a general framework, the reality of living with pancreatitis — particularly for women — can be considerably more nuanced. Female pancreatitis pain location may be the same as in men anatomically, but the way that pain is experienced, described, and even recognized by healthcare providers can differ significantly based on sex-specific factors.
Understanding the female experience of pancreatitis pain is important for several reasons. Women face unique risk factors — particularly gallstone formation driven by hormonal influences, pregnancy, and the use of oral contraceptives — that make them more susceptible to certain forms of pancreatitis. Additionally, research across many medical conditions has consistently shown that women's pain is more frequently underestimated, misattributed, or delayed in diagnosis compared to men's pain presenting with the same underlying condition.
This guide is designed to provide a thorough, female-centered understanding of pancreatitis pain: where it is located, how it radiates, how it may be modified by hormonal and anatomical factors, how it overlaps with other conditions common in women, and what women should know to advocate effectively for themselves when seeking care. Whether you have been diagnosed with pancreatitis, are experiencing unexplained abdominal pain, or want to understand this condition more deeply, this guide offers the specific, actionable knowledge you need.
The Primary Pain Location: Upper Left Abdomen
The pancreas sits in the retroperitoneum — behind the stomach and in front of the spine — spanning from the upper left side of the abdomen (where the pancreatic tail lies near the spleen) to the center-right (where the pancreatic head is nestled in the curve of the duodenum). This anatomical location directly determines where female pancreatitis pain is felt.
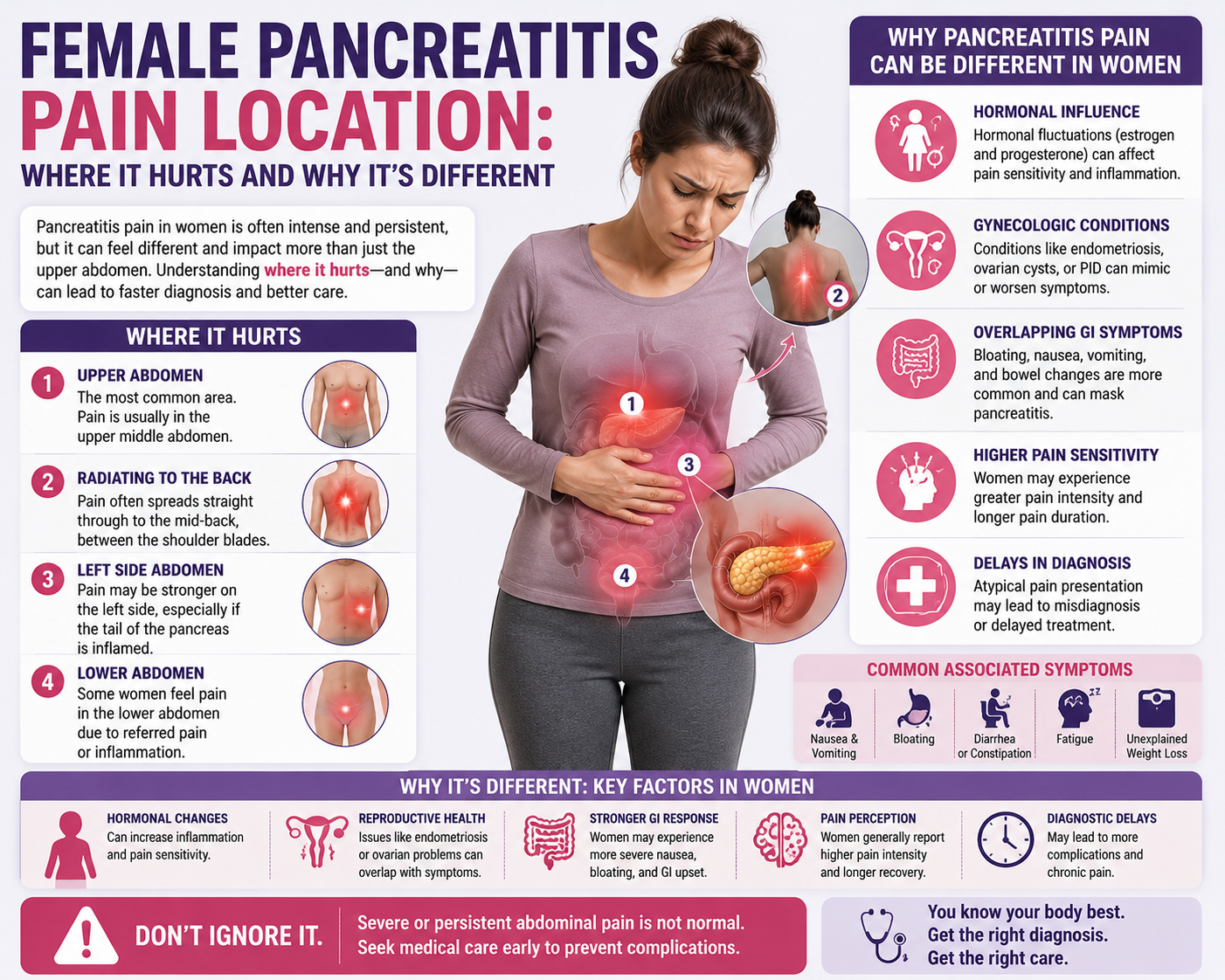
In both men and women, the primary location of pancreatitis pain is the epigastric region — the central upper abdomen, directly below the breastbone (sternum) and above the navel. This area corresponds roughly to the location of the pancreatic body, which is the central portion of the organ most commonly affected by inflammation. Many patients describe the pain as originating deep in the abdomen, with a quality that is difficult to localize precisely — not a sharp, surface-level sensation but a profound, visceral ache that seems to come from within the body.
In a significant proportion of cases (roughly half), the pain extends to the left upper quadrant — the area just below the left ribcage. This reflects involvement of the pancreatic tail or spread of inflammation to the surrounding tissues. Pain may also be felt in the right upper quadrant, particularly when gallstone obstruction is the underlying cause and the bile duct (which runs through the head of the pancreas on the right side) is involved. Some women report that the pain feels diffuse across the entire upper abdomen rather than sharply localized to one spot.

The Back: A Critical Pain Radiation Pattern
One of the most diagnostically important features of pancreatitis pain — in both women and men — is its tendency to radiate to the back. In approximately 50% of patients, the pain does not stay confined to the abdomen but wraps around the body, producing a band-like sensation that extends from the upper abdomen to the mid-back or the area between the shoulder blades. This radiation occurs because the pancreas, sitting in the retroperitoneum, is intimately connected to nerves and tissues that extend to the back, and as inflammation spreads, these posterior structures become involved.
For women, this back pain can be particularly confusing because back pain is extremely common for other reasons in the female population: musculoskeletal strain, menstrual-related pain (dysmenorrhea), ovarian cysts, and kidney problems can all cause back pain that overlaps anatomically with the back pain of pancreatitis. This overlap is one reason why pancreatitis is sometimes delayed in diagnosis in women — the back pain component may be attributed to a musculoskeletal issue or dismissed as period-related discomfort rather than being recognized as part of a pancreatic pain syndrome.
The character of pancreatic back pain is typically described as a deep, constant ache that is not relieved by changing position. This distinguishes it from the positional back pain of musculoskeletal origin, which typically improves with rest, certain positions, or over-the-counter pain medications. A woman who experiences severe upper abdominal pain together with persistent mid-back pain — especially if these symptoms follow a fatty meal or an episode of heavy drinking — should seek immediate medical evaluation for pancreatitis.
How Hormonal Factors Shape the Female Pain Experience
The female hormonal environment has a profound influence on both the causes and the experience of pancreatitis pain. Estrogen and progesterone — the primary female sex hormones — affect gallbladder function and bile composition in ways that directly increase gallstone formation risk, making women two to three times more likely than men to develop gallstones and gallstone-related pancreatitis. Estrogen increases cholesterol secretion into bile while progesterone slows gallbladder emptying, both of which promote cholesterol crystallization and stone formation.
Pregnancy amplifies these hormonal effects significantly. Pregnant women have substantially elevated estrogen and progesterone levels, a further slowing of gallbladder motility, and a reduction in gallbladder emptying efficiency. These changes make pregnancy a well-recognized risk period for gallstone formation and gallstone pancreatitis, with pancreatitis complicating approximately 1 in 1,000 to 1 in 10,000 pregnancies. The pain location in pregnancy is similar to that in non-pregnant women, though the growing uterus may shift the position of abdominal organs slightly and make physical examination more challenging.
Oral contraceptive use and hormone replacement therapy also influence pancreatitis risk in women. Exogenous estrogens increase triglyceride levels, which can contribute to hypertriglyceridemia-induced pancreatitis in susceptible individuals. Additionally, oral contraceptives can increase gallstone formation risk. Women taking hormonal preparations who experience unexplained abdominal pain should discuss pancreatitis screening with their healthcare provider.
Overlapping Pain Conditions in Women: The Diagnostic Challenge
One of the most significant challenges in recognizing female pancreatitis pain location is the extensive overlap between pancreatitis and several other conditions that are common in women. These conditions can mimic pancreatitis, coexist with it, or even be confused for it by clinicians who are not thinking broadly enough about the differential diagnosis.
Irritable bowel syndrome (IBS) affects women at twice the rate of men and commonly causes upper and lower abdominal pain, bloating, nausea, and altered bowel habits — all symptoms that can overlap with pancreatitis. Ovarian cysts and ovarian torsion (twisting of the ovary) can cause severe lower or lateral abdominal pain that may radiate to the back, sometimes presenting with nausea and vomiting in a pattern that superficially resembles acute pancreatitis. Pelvic inflammatory disease (PID) causes lower abdominal and pelvic pain, but severe cases can produce upper abdominal discomfort as well. Endometriosis — a condition in which endometrial tissue grows outside the uterus — can cause cyclic and non-cyclic abdominal and back pain of variable location and intensity.
Gallbladder disease (including cholecystitis and biliary colic) is frequently confused with pancreatitis and can also cause it. Biliary colic produces right upper quadrant pain that may radiate to the right shoulder or back, typically following a fatty meal. Since gallstones are a common cause of both biliary colic and acute pancreatitis, these conditions frequently coexist and can be difficult to distinguish without laboratory testing. The presence of an elevated serum lipase — three times the upper limit of normal — is the biochemical hallmark that distinguishes pancreatitis from uncomplicated gallbladder disease.

Specific Pain Characteristics Women Report
Beyond the anatomical location, the qualitative characteristics of female pancreatitis pain can provide important diagnostic clues. Women with acute pancreatitis most commonly describe the pain as severe to excruciating in intensity — often rating it 8–10 on a 10-point pain scale at its peak. The onset is typically rapid, often described as coming on within 15–30 minutes and quickly reaching a crescendo of intensity. Unlike the intermittent, cramping pain of bowel conditions, pancreatitis pain is generally constant and does not come and go in rhythmic waves.
Women frequently report that the pain is worsened by eating, drinking, or deep breathing. Lying flat often intensifies the discomfort, while leaning forward in a seated position or curling into the fetal position may provide slight relief — a position-related pattern that is clinically recognized as a useful indicator of retroperitoneal organ involvement. The mere sight or smell of food may be deeply aversive due to the concurrent nausea that almost universally accompanies the pain of acute pancreatitis.
Some women describe a sense of pressure or heaviness in the upper abdomen, as though something is pushing or pressing from the inside. This sensation may relate to the abdominal distension caused by ileus (bowel paralysis) and fluid accumulation around the inflamed pancreas. The abdomen may feel tender to the touch, and even minor pressure — from clothing waistbands, or a partner's arm during sleep — can be intensely painful during an acute attack.
Pancreatitis Pain During Pregnancy: Location and Special Concerns
Pancreatitis during pregnancy presents particular diagnostic challenges because many normal pregnancy symptoms — nausea, vomiting, abdominal discomfort, and altered appetite — overlap with pancreatitis symptoms. The pain location in pregnant women is similar to that in non-pregnant patients: predominantly epigastric, often radiating to the back. However, as the pregnancy progresses, the enlarging uterus displaces abdominal organs upward and outward, potentially modifying the perceived location of pain and complicating physical examination findings.
Pancreatitis in pregnancy is most common during the third trimester, when gallstone formation risk is highest and triglyceride levels are naturally elevated. Prompt diagnosis is essential because severe pancreatitis in pregnancy is associated with serious complications for both mother and fetus, including preterm labor, premature delivery, fetal distress, and in very severe cases, maternal and fetal mortality. Any pregnant woman experiencing severe upper abdominal pain should be evaluated emergently for pancreatitis with serum lipase measurement and ultrasound.
When Pancreatitis Pain Becomes Chronic: Female Experience
In women who develop chronic pancreatitis — either from recurrent acute episodes or from progressive underlying damage — the pain pattern can change substantially compared to acute pancreatitis. Chronic pancreatitis pain in women is typically centered in the same upper abdominal region but may become more persistent, less episodic, and more difficult to characterize. It may be described as a dull, aching, or gnawing discomfort that is present most or all of the time, punctuated by more severe flares.
Women with chronic pancreatitis may also experience pain that worsens after eating — a phenomenon called postprandial pain — which can lead to avoidance of food and severe unintentional weight loss. The fear of food-triggered pain is psychologically distressing and can contribute to anxiety, depression, and social isolation, all of which are disproportionately reported in female patients with chronic pancreatitis. Nutritional deficiency from both malabsorption (due to pancreatic exocrine insufficiency) and inadequate intake compounds the physical deterioration.
The psychological dimension of chronic pain in women deserves specific attention. Studies have shown that women's pain reports are more likely than men's to be attributed to psychological or emotional causes rather than to organic disease. Women with chronic pancreatitis may face dismissal of their symptoms as anxiety, somatization, or drug-seeking behavior, particularly in the context of opioid prescribing for severe pain. Awareness of these disparities helps women advocate for themselves and seek providers who take their pain seriously.

What Women Should Know About Seeking Diagnosis
If you are a woman experiencing upper abdominal pain that may be consistent with female pancreatitis pain location, several steps can help ensure timely and accurate diagnosis. First, document your pain precisely: note the location (upper abdomen, back, side), the character (sharp, dull, burning, aching), the timing (sudden onset, gradual, constant, intermittent), the severity on a 1–10 scale, any triggers (eating, particularly fatty foods; alcohol consumption; physical activity), any relieving factors (fasting, positioning), and any associated symptoms (nausea, vomiting, fever, jaundice, changes in stool or urine color).
When presenting to a healthcare provider, be specific and persistent. Do not allow your symptoms to be dismissed without biochemical evaluation — a simple blood test for serum lipase (and amylase) is the standard first-line test for pancreatitis and should be ordered whenever pancreatitis is a diagnostic consideration. An abdominal ultrasound is also commonly performed to evaluate for gallstones. If initial tests are inconclusive but your symptoms are severe, request further evaluation including CT imaging of the abdomen.
Insist on a comprehensive evaluation for the underlying cause of pancreatitis, particularly if you have had more than one episode. Causes including gallstones, hypertriglyceridemia, genetic mutations, and autoimmune pancreatitis all require different management strategies. Treating the underlying cause is essential for preventing recurrence and the progression to chronic pancreatitis.
Prevention Strategies Specific to Women
Women can take several proactive steps to reduce their risk of pancreatitis, particularly by addressing the sex-specific risk factors discussed throughout this guide. Maintaining a healthy body weight is the single most impactful preventive measure for gallstone-related pancreatitis, as obesity is the leading modifiable risk factor for gallstone formation. Avoiding rapid weight loss (which paradoxically increases gallstone risk by mobilizing large amounts of cholesterol into bile) is equally important — weight loss should be gradual, aiming for no more than 1–2 pounds per week.
Women using oral contraceptives or hormone replacement therapy should be aware of their potential to elevate triglycerides, particularly in women who already have elevated baseline levels or a family history of hypertriglyceridemia. Regular monitoring of lipid levels is advisable for women on long-term hormonal therapy. During pregnancy, dietary fat should be moderated, and any upper abdominal pain should be evaluated promptly. Women with a history of pancreatitis who become pregnant should inform their obstetric team so that appropriate monitoring can be arranged.
Conclusion
Female pancreatitis pain location follows the same fundamental anatomical principles as pancreatitis pain in men — centered in the upper abdomen, often radiating to the back, and associated with nausea, vomiting, and systemic inflammation. However, the female experience of this condition is shaped by a unique constellation of hormonal factors, sex-specific risk contributors, overlapping gynecological conditions, and documented disparities in clinical recognition and treatment. Understanding these dimensions empowers women to recognize their symptoms accurately, communicate them effectively to healthcare providers, and advocate for the thorough, evidence-based care they deserve. If you experience severe upper abdominal pain with or without back radiation, do not wait — seek emergency evaluation and ensure that pancreatitis is specifically tested for and either confirmed or excluded.