Gallbladder Stones: The Silent Digestive Condition That Can Suddenly Become an Emergency

Medical Disclaimer: This educational article does not replace medical diagnosis or emergency care. Severe abdominal pain, jaundice, chest pressure, breathing difficulty, fever, or persistent vomiting should always be evaluated by a qualified healthcare professional immediately.
Most people never think about their gallbladder until something goes wrong.
The organ itself is small, hidden beneath the liver, and almost invisible in daily life. Yet gallbladder stones can suddenly transform an ordinary dinner into hours of severe pain, nausea, sweating, or even a surgical emergency.
What makes gallstone disease uniquely dangerous is unpredictability.
A person may carry gallstones silently for years without symptoms. Then, after a single fatty meal, one tiny crystal can shift position, block a narrow duct, and trigger a cascade of inflammation, pressure buildup, infection, or pancreatitis.
Some patients assume they have acid reflux. Others believe it is muscle strain or food poisoning. In certain cases, symptoms may even resemble a heart attack.
This guide explains how gallbladder stones form, why some remain harmless while others become dangerous, how attacks develop mechanically inside the body, and which symptoms should never be ignored.
Emergency Warning Signs That Require Immediate Medical Care
Seek urgent medical evaluation if gallbladder-related symptoms occur with:
- Fever or shaking chills
- Yellowing of the eyes or skin
- Dark urine
- Pale or clay-colored stools
- Persistent vomiting
- Severe pain lasting longer than 5–6 hours
- Shortness of breath
- Chest heaviness
- Cold sweats
- Sudden weakness or confusion
These symptoms may indicate:
- Acute gallbladder inflammation
- Bile duct obstruction
- Gallstone pancreatitis
- Ascending cholangitis
- Sepsis
- Cardiac emergencies mistaken for digestive pain
Important Safety Note
Do not attempt internet “gallbladder flushes” during an active attack.
Do not apply intense heat directly to the abdomen.
Avoid masking symptoms with excessive pain medication before medical evaluation, since this may delay accurate emergency diagnosis.
Understanding the Gallbladder’s Job
The gallbladder acts as a bile storage reservoir.
The liver continuously produces bile throughout the day, but the body does not always need large amounts immediately.
Instead of sending bile directly into the intestine nonstop, the gallbladder:
- Stores bile
- Concentrates bile
- Releases bile during meals
This process helps digest dietary fat efficiently.
What Is Bile Made Of?
Bile is a complex digestive fluid containing:
- Cholesterol
- Bile salts
- Lecithin
- Water
- Bilirubin
- Electrolytes
Under normal conditions, these ingredients remain chemically balanced.
Gallstones begin forming when that balance becomes unstable.
Gallstones Are Crystals Before They Become “Stones”
Most patients imagine gallstones as pebbles that suddenly appear.
In reality, the process usually begins microscopically.
Tiny cholesterol crystals gradually form inside stagnant or chemically overloaded bile.
Over time:
- Crystals cluster together
- Sludge develops
- Hardened deposits enlarge
- Gallstones emerge
This process may continue silently for years before symptoms begin.
The “Overloaded Iced Tea” Analogy
A simple way to understand gallstone formation is to imagine sweet iced tea.
At first:
- Sugar dissolves normally
Eventually:
- The liquid becomes oversaturated
- Excess sugar settles
- Crystals form at the bottom
Gallstones form through a similar biochemical process.
When cholesterol concentration exceeds the dissolving capacity of bile salts, crystals begin precipitating from the fluid itself.
Types of Gallbladder Stones
Gallstones are not all chemically identical.
Different stone types develop through different biological pathways.
Cholesterol Stones
These are the most common stones in the United States.
They are typically:
- Yellow-green
- Smooth
- Cholesterol-rich
They form when:
- The liver secretes excessive cholesterol
- Gallbladder emptying slows
- Bile becomes concentrated
Pigment Stones
Pigment stones are darker and composed largely of bilirubin compounds.
They are more commonly associated with:
- Liver disease
- Biliary infections
- Cirrhosis
- Chronic hemolytic disorders
These stones often appear:
- Black
- Brown
- Brittle
- Irregular
Visual Recommendation: Add a side-by-side infographic comparing cholesterol stones vs pigment stones, including appearance, composition, and associated conditions.
Why Tiny Gallstones Can Be More Dangerous Than Large Ones
One of the biggest misconceptions surrounding gallstones is the idea that larger stones automatically create greater danger.
Mechanically, the opposite may sometimes be true.
Small Stones and Biliary Sludge
Tiny stones under 5 mm possess extremely high mobility.
Because they move easily, they may escape the gallbladder entirely and travel into narrow ducts.
This can create sudden blockage inside:
- The common bile duct
- The pancreatic duct
- The ampulla region
Small stones therefore carry higher risk for:
- Acute pancreatitis
- Obstructive jaundice
- Infection
- Emergency hospitalization
Gallstone Pancreatitis: A Dangerous Chain Reaction
The pancreas releases powerful digestive enzymes.
When a migrating stone blocks pancreatic drainage:
- Enzymes become trapped
- Internal inflammation escalates rapidly
- Pancreatic tissue begins digesting itself
This condition can become life-threatening quickly.
Symptoms often include:
- Severe upper abdominal pain
- Persistent vomiting
- Sweating
- Pain radiating toward the back
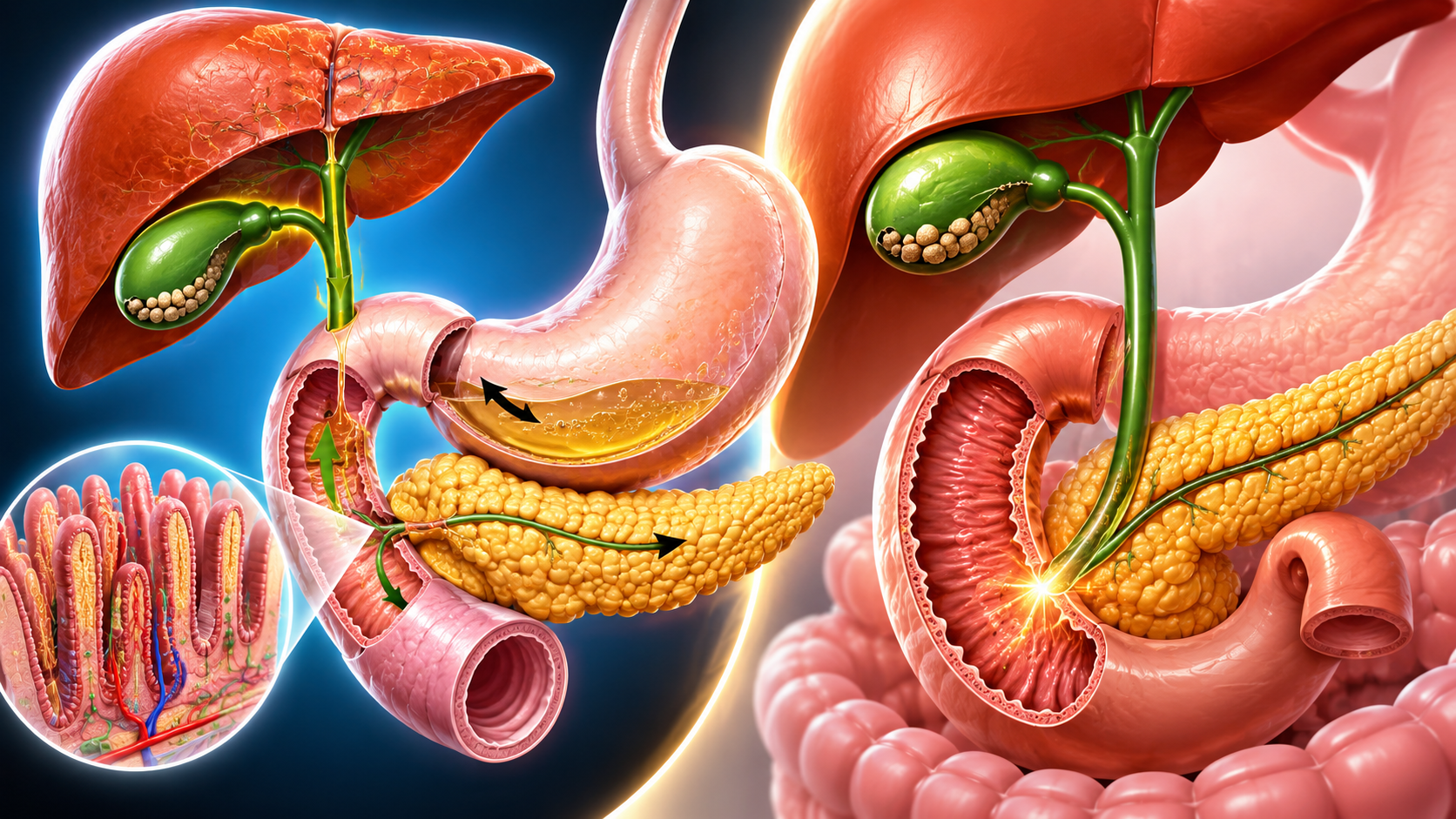
Visual Recommendation: Insert a “micro-stone obstruction pathway” illustration showing how a tiny stone blocks the pancreatic duct junction.
Large Stones Create Different Risks
Large stones usually cannot travel easily into narrow ducts.
However, they may create chronic irritation inside the gallbladder itself.
Over years, repeated friction can contribute to:
- Gallbladder wall thickening
- Chronic inflammation
- Fibrosis
- Mechanical dysfunction
- More difficult surgery later
Some large stones eventually reach golf-ball size.
Why Gallstones Form in Certain People
Gallstones develop through a combination of:
- Hormonal influences
- Metabolic factors
- Digestive mechanics
- Genetic predisposition
- Bile stagnation
The “4 Fs” Risk Pattern
Doctors sometimes summarize common gallstone risk factors using the traditional “4 Fs” framework:
- Female
- Forty
- Fertile
- Fat
While simplistic, this pattern reflects broad epidemiological trends seen in digestive medicine.
Estrogen and Gallbladder Disease
Estrogen increases cholesterol secretion into bile.
Progesterone slows gallbladder contractions.
Together, these hormonal effects may encourage:
- Biliary stasis
- Sludge formation
- Crystal precipitation
This helps explain why gallstones occur more frequently during:
- Pregnancy
- Hormone therapy
- Certain contraceptive use
Why Pregnancy Changes Gallbladder Function
Pregnancy alters digestive physiology dramatically.
Hormonal shifts slow bile flow, while the enlarging uterus changes abdominal organ positioning.
This combination may produce:
- Slower gallbladder emptying
- Increased cholesterol concentration
- More bile stagnation
Symptoms during pregnancy may also appear atypically.
Rapid Weight Loss and Crash Dieting
Aggressive dieting represents one of the strongest modern gallstone triggers.
When body fat breaks down rapidly:
- Large amounts of cholesterol enter bile
- Gallbladder chemistry destabilizes
- Crystal formation accelerates
Clinical digestive observations commonly associate higher gallstone risk with sustained weight loss exceeding approximately 1.5 kg (3.3 pounds) weekly.
This relationship has been repeatedly observed in digestive medicine because rapid fat metabolism overloads bile with cholesterol faster than bile salts can safely dissolve it.
Intermittent Fasting and the “Gallbladder Freeze” Mechanism
Intermittent fasting itself is not inherently harmful for most healthy individuals.
However, prolonged fasting combined with extremely low dietary fat may reduce gallbladder contractions substantially in susceptible people.
This issue appears most relevant in individuals who already have:
- Sludge
- Pre-existing stones
- Impaired gallbladder emptying
- Biliary dyskinesia
Without regular stimulation from food:
- Cholecystokinin (CCK) release falls
- Gallbladder contractions weaken
- Bile sits stagnant longer
- Cholesterol precipitation may accelerate
Some specialists describe this process as the “Gallbladder Freeze” effect.
Why Fatty Meals Trigger Attacks
Many patients notice attacks begin shortly after greasy meals.
This relationship is deeply mechanical.
The Role of Cholecystokinin (CCK)
When dietary fat enters the intestine:
- The digestive system releases CCK
- The gallbladder contracts forcefully
- Concentrated bile is squeezed into bile ducts
If a stone blocks the pathway during contraction:
- Pressure rises rapidly
- The gallbladder stretches painfully
- A biliary attack begins
Common triggers include:
- Fried foods
- Heavy cream sauces
- Bacon
- Pizza
- Fast food
- Large late-night meals
Visual Recommendation: Insert an anatomical diagram showing gallbladder contraction against a blocked duct.
What a Gallbladder Attack Feels Like
Patients frequently describe gallbladder pain differently from normal stomach pain.
The discomfort often feels:
- Deep
- Internal
- Steady
- Difficult to pinpoint
Some patients describe it as:
“A fist pushing underneath my ribs.”
Common Attack Symptoms
Symptoms may include:
- Right upper abdominal pain
- Pressure beneath the ribs
- Shoulder blade pain
- Nausea
- Vomiting
- Sweating
- Restlessness
Unlike gas cramps, gallbladder pain usually does not improve quickly with stretching or bowel movements.
Why Pain Travels Into the Shoulder and Back
This phenomenon is called referred pain.
Inflammation near the diaphragm irritates nerve pathways that communicate with the shoulder region.
As a result, the brain interprets the signal incorrectly and perceives pain farther away from the gallbladder itself.
Visual Recommendation: Add a body-map infographic showing pain radiation into the shoulder blade and upper back.
Why Attacks Often Happen at Night
Nighttime attacks are extremely common.
Several physiological factors may contribute.
Heavy Evening Meals
Dinner often contains the highest fat load of the day.
Hours later, strong gallbladder contractions may still occur during sleep.
The Gravity Effect
When standing upright:
- Stones may settle harmlessly at the bottom of the gallbladder
When lying flat:
- The gallbladder shifts position
- Stones roll more freely
- Obstruction risk increases
This mechanical explanation aligns closely with real-world patient experiences during midnight attacks.
Gallstones vs Acid Reflux vs Heart Attack
Upper abdominal pain can be medically confusing.
Gallbladder Attack
More commonly associated with:
- Right upper abdominal pain
- Pain after fatty meals
- Shoulder blade radiation
- Nausea
- Persistent pressure
Acid Reflux (GERD)
More commonly associated with:
- Burning sensation
- Sour taste
- Symptoms worsening while lying down
- Relief from antacids
Heart Attack
Cardiac emergencies may produce:
- Chest heaviness
- Cold sweats
- Shortness of breath
- Jaw pain
- Dizziness
- Upper abdominal pressure
Critical Note
Because a large fatty meal forces the heart to work harder to redirect blood flow toward digestion, it can occasionally trigger cardiac symptoms in vulnerable individuals.
If upper abdominal pressure occurs alongside sweating, breathing difficulty, dizziness, or weakness, especially in people with cardiovascular risk factors, assume it may represent a cardiac emergency until evaluated by emergency professionals.
Older adults, women, and diabetic patients may experience heart attacks without classic chest pain.
Diabetes and “Silent” Gallbladder Emergencies

Gallbladder disease may behave differently in long-standing diabetes.
Autonomic neuropathy can blunt visceral pain signals.
As a result, dangerous infection or inflammation may progress without dramatic pain.
Instead, symptoms may appear as:
- Weakness
- Fever
- Nausea
- Malaise
- Appetite loss
This makes delayed diagnosis more likely.
How Gallstones Are Diagnosed
Doctors combine symptoms, examination findings, and imaging studies.
Ultrasound
Ultrasound remains the primary diagnostic tool.
It can detect:
- Stones
- Sludge
- Gallbladder inflammation
- Duct enlargement
- Wall thickening
Gallstones frequently produce an imaging effect called acoustic shadowing.
HIDA Scan
A HIDA scan evaluates gallbladder function rather than simply structure.
This test becomes especially useful when:
- Symptoms strongly suggest gallbladder disease
- Ultrasound appears normal
Low ejection fraction results may indicate:
- Biliary dyskinesia
- Functional gallbladder disorders
ERCP
ERCP allows specialists to:
- Visualize bile ducts
- Remove trapped stones
- Relieve dangerous obstruction
This procedure can become lifesaving during emergencies.
Modern Treatment Options
Treatment depends on:
- Symptoms
- Stone size
- Complication risk
- Obstruction severity
- Infection status
Silent Gallstones Often Require No Treatment
Many gallstones remain asymptomatic forever.
If stones are not causing:
- Pain
- Infection
- Obstruction
- Inflammation
watchful waiting is often medically appropriate.
Laparoscopic Gallbladder Surgery
Laparoscopic cholecystectomy is considered the modern gold standard treatment for symptomatic gallstones.
The procedure removes the entire gallbladder through several tiny incisions.
Most patients:
- Return home quickly
- Resume light activity within days
- Recover substantially within 1–2 weeks
Why Surgeons Remove the Whole Gallbladder
Patients often ask why surgeons do not simply remove individual stones.
The reason is functional.
The gallbladder itself usually has underlying dysfunction that allowed stones to form initially.
If only stones are removed:
- New stones frequently develop again
Removing the organ prevents recurrence more effectively.
Can You Live Normally Without a Gallbladder?
Yes.
The liver continues producing bile even after surgery.
Without a storage reservoir:
- Bile flows continuously into the intestine instead of being stored
Some patients temporarily notice:
- Loose stools
- Bloating
- Fat sensitivity
Most adapt over time.
Why Internet “Gallbladder Flushes” Are Misleading
Online detox trends involving olive oil and lemon juice remain extremely popular.
However, these methods are not scientifically validated treatments for true gallstones.
The “Fake Stone” Phenomenon
The soft green clumps passed after these cleanses are usually not real gallstones.
Instead, they are often fatty soap-like compounds created through chemical reactions between:
- Oil
- Acid
- Digestive substances
This process resembles saponification rather than true stone elimination.
Why Flushes Can Become Dangerous
If real gallstones exist, aggressive oil loading may force stones into narrow ducts.
This can trigger:
- Obstruction
- Infection
- Pancreatitis
- Emergency surgery
Frequently Asked Questions
Can gallstones disappear naturally?
Most developed gallstones do not dissolve spontaneously. However, silent stones may remain harmless for years without causing symptoms.
Why are small gallstones dangerous?
Small stones move more easily and may block critical ducts connected to the liver or pancreas.
Can fasting cause gallstones?
Prolonged fasting combined with impaired gallbladder emptying may increase bile stagnation in susceptible individuals, especially those with pre-existing sludge or stones.
Is surgery always necessary?
No. Silent gallstones often require monitoring rather than immediate surgery.
Can people live normally without a gallbladder?
Yes. Most patients eventually return to normal lifestyles after recovery.
Conclusion
Gallbladder stones are far more complex than simple “digestive rocks.”
They involve a combination of:
- Cholesterol chemistry
- Hormonal influences
- Mechanical obstruction
- Digestive physiology
- Inflammatory risk
Some stones remain silent indefinitely.
Others suddenly migrate into narrow ducts and trigger severe emergencies involving pancreatitis, infection, or obstruction.
Understanding the warning signs, attack patterns, dietary triggers, and emergency symptoms may help patients seek treatment before complications become dangerous.
Persistent upper abdominal pain should never be dismissed casually, especially when accompanied by fever, jaundice, vomiting, breathing difficulty, or chest pressure.