Gallstones: A Complete Guide to Symptoms, Causes, and Modern Treatment

Medically Reviewed Educational Content
Audience: U.S. readers seeking medically accurate digestive health information.
Medical Disclaimer: This article is educational and informational only. It should not replace professional medical diagnosis, emergency evaluation, or treatment advice from a licensed healthcare provider.
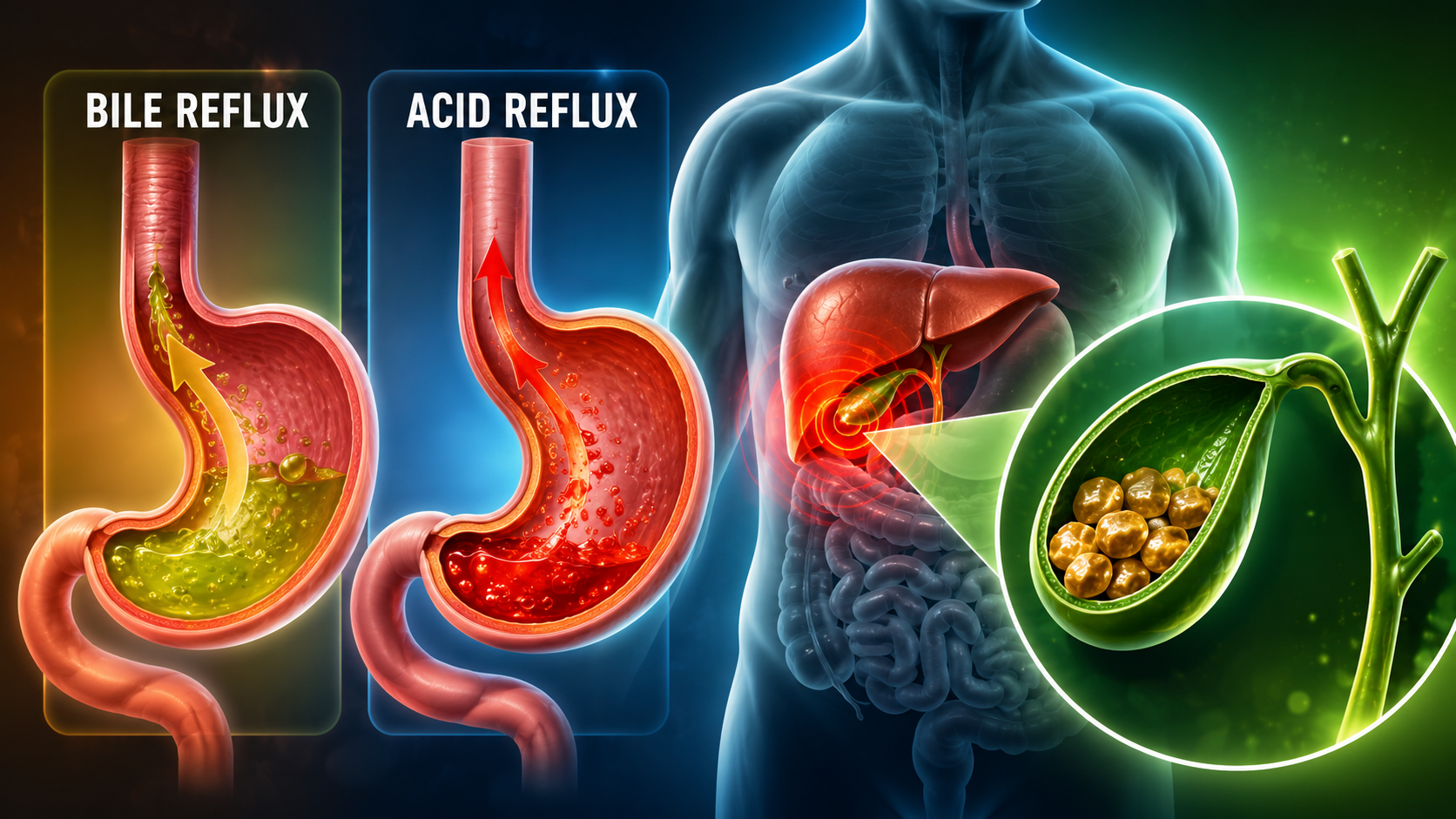
Gallstones are hardened digestive deposits that form inside the gallbladder and can range from harmless “silent stones” to severe medical emergencies involving infection, pancreatitis, or bile duct obstruction. Some people discover gallstones during a routine ultrasound for an unrelated issue, while others experience sudden attacks of crushing upper abdominal pain that feel frighteningly similar to a heart attack.
One reason gallbladder disease causes so much confusion is because the symptoms often imitate acid reflux, indigestion, gastritis, muscle strain, or even cardiac problems. A small stone may sit quietly for years before suddenly shifting into a narrow bile duct after a fatty meal, triggering pressure, inflammation, nausea, and severe digestive distress.
This medically reviewed guide explains how gallstones form, what a gallbladder attack feels like, why symptoms often happen at night, and when emergency care becomes necessary.
Emergency Red Flags: When Gallstones Become Dangerous
Seek immediate medical evaluation if symptoms occur alongside:
- Fever or shaking chills
- Yellowing of the skin or eyes (jaundice)
- Dark urine
- Pale or clay-colored stools
- Persistent vomiting
- Severe pain lasting more than 5–6 hours
- Chest heaviness
- Shortness of breath
- Fainting or sudden weakness
These symptoms may indicate:
- Acute cholecystitis
- Gallstone pancreatitis
- Bile duct obstruction
- Ascending cholangitis
- Sepsis-related complications
The Heart Attack Warning Many Patients Miss
Gallbladder pain and cardiac pain can overlap in dangerous ways.
Many patients assume upper abdominal pain after a large meal must be “indigestion” or gallstones, when in reality it may represent reduced blood flow to the heart.
Critical Clinical Note
A heavy, high-fat meal increases the body’s circulatory demands and may trigger severe angina or a heart attack in patients with underlying cardiovascular disease.
If upper abdominal pressure occurs with:
- Sweating
- Breathlessness
- Jaw pain
- Chest tightness
- Sudden weakness
- Dizziness
seek emergency care immediately rather than assuming it is “just gallstones.”
This warning is especially important for:
- Older adults
- Women
- Diabetic patients
- Individuals with known heart disease
In these groups, heart attacks may present primarily as upper abdominal discomfort rather than classic crushing chest pain.
Understanding Gallstones: What Are They?
Gallstones are hardened crystal-like deposits that develop inside the gallbladder, a small digestive organ located beneath the liver.
The gallbladder stores bile, a digestive fluid responsible for helping the body digest fats after meals.
Bile contains:
- Cholesterol
- Bile salts
- Bilirubin
- Lecithin
- Water
Under normal conditions, these components remain chemically balanced and dissolved. Problems begin when the balance changes and crystals start forming inside stagnant or overly concentrated bile.
Visual Recommendation: Anatomy diagram highlighting the liver, gallbladder, pancreas, and common bile duct.
The Chemistry Behind Gallstones (The “Sludge” Phase)
Gallstones rarely appear overnight.
Most begin as microscopic cholesterol crystals suspended inside thickened bile.
As cholesterol concentration increases beyond what bile salts can safely dissolve:
- Tiny crystals precipitate
- Thick biliary sludge develops
- Sludge clusters together
- Stones gradually harden over time
A helpful analogy involves adding excessive sugar into iced tea. Initially, the sugar dissolves normally. Eventually the liquid becomes oversaturated, and crystals settle at the bottom. Gallstones form through a similar biochemical process.
Cholesterol Gallstones
These are the most common type in the United States and are usually:
- Yellow-green
- Smooth
- Cholesterol-rich
They form when the liver releases more cholesterol into bile than the digestive system can safely keep dissolved.
Pigment Gallstones
Pigment stones are darker and more brittle.
They are commonly associated with:
- Liver cirrhosis
- Chronic biliary infections
- Conditions involving accelerated red blood cell breakdown
Pigment stones often appear:
- Black
- Dark brown
- Irregular
- Fragile
Silent Gallstones vs Symptomatic Gallstones

One of the most surprising facts about gallbladder disease is that many people never develop symptoms at all.
These are called silent gallstones.
Silent stones:
- Stay inside the gallbladder
- Do not significantly obstruct bile flow
- Cause little inflammation
Because of this, many physicians recommend a “watchful waiting” approach rather than immediate surgery when asymptomatic stones are discovered incidentally.
Finding gallstones on an ultrasound does not automatically mean surgery is required.
Symptoms typically begin when a stone temporarily blocks a duct or causes inflammation.
Recognizing the Symptoms of Gallstones
Gallstone symptoms vary widely depending on:
- Stone size
- Degree of obstruction
- Presence of inflammation
- Gallbladder motility
- Involvement of nearby organs
Some people experience only mild digestive discomfort. Others develop sudden severe attacks requiring emergency care.
Biliary Colic: The “Gallbladder Attack”
The classic gallbladder attack is medically known as biliary colic.
This occurs when a stone temporarily blocks the cystic duct while the gallbladder contracts.
After eating fatty food, the digestive hormone cholecystokinin (CCK) signals the gallbladder to squeeze bile into the intestine.
If a stone blocks the exit pathway during contraction:
- Pressure builds rapidly
- The gallbladder stretches painfully
- Inflammation develops
- Severe discomfort follows
Unlike gas pain, biliary colic usually feels:
- Deep
- Steady
- Internal
- Pressure-like
- Difficult to pinpoint precisely
Many patients describe the sensation as:
“A fist pressing underneath my ribs.”
The pain commonly:
- Peaks within 30–60 minutes
- Persists steadily for several hours
- Develops after fatty meals
- Appears late at night
Visual Recommendation: Diagram showing a gallstone physically blocking the cystic duct.
Gallbladder Pain Location: Where Does It Hurt?
The classic pain location involves the:
- Right upper abdomen (RUQ)
- Area beneath the right rib cage
- Upper middle abdomen beneath the breastbone
However, gallbladder pain often spreads beyond this region.
Referred Pain: Why the Shoulder and Back Hurt
Gallbladder attacks frequently create referred pain, meaning discomfort is felt far from the gallbladder itself.
Common referred pain locations include:
- Right shoulder blade
- Between the shoulder blades
- Upper back
- Right shoulder
This happens because inflammation near the diaphragm irritates the phrenic nerve, which shares neurological pathways with the shoulder region.
The brain interprets these signals incorrectly and “projects” pain elsewhere.
Many patients initially believe they injured a back muscle before discovering the gallbladder is responsible.
Visual Recommendation: Pain mapping infographic showing radiation from the RUQ toward the scapula and right shoulder.
Non-Painful Symptoms Many People Ignore
Not all gallbladder symptoms involve dramatic pain.
Some individuals primarily experience chronic digestive complaints such as:
- Bloating
- Burping
- Nausea
- Fat intolerance
- Feeling overly full after meals
- Mild upper abdominal pressure
Because these symptoms overlap heavily with acid reflux and gastritis, many people delay medical evaluation for months or years.
Gallstones vs GERD vs Indigestion
Gallbladder Symptoms Often Cause:
- Deep pressure beneath the ribs
- Pain after fatty meals
- Shoulder blade radiation
- Nausea lasting hours
- Symptoms not relieved by antacids
GERD More Commonly Causes:
- Burning behind the breastbone
- Acid taste in the throat
- Symptoms worsening while lying flat
- Temporary relief with antacids
Gas Pain More Commonly Causes:
- Sharp moving cramps
- Relief after passing gas
- Temporary abdominal distention
- Shifting pain locations
Gallbladder pain generally feels more “deep and squeezing,” while GERD feels “burning.”
Visual Recommendation: Comparison chart — Gallstones vs GERD vs Gas Pain vs Heart Attack.
Why Gallbladder Attacks Often Happen at Night
Many patients report waking suddenly after midnight with severe symptoms.
Several physiological mechanisms may contribute.
Heavy Evening Meals
Dinner is often the largest and fattiest meal of the day, forcing stronger gallbladder contractions.
Slower Overnight Digestion
Digestive motility naturally slows during sleep, potentially increasing bile stagnation.
The “Gravity Effect”
One of the most clinically interesting explanations involves body positioning.
While standing upright:
- Stones may settle harmlessly at the bottom of the gallbladder
When lying flat:
- The gallbladder shifts orientation
- Stones drift toward the narrow neck
- Temporary blockage becomes more likely
This explanation closely matches many patient experiences and helps explain why attacks commonly begin after going to bed.
Emergency Complications of Gallstones
Most uncomplicated gallbladder attacks eventually improve.
Persistent symptoms may indicate severe complications requiring emergency treatment.
Acute Cholecystitis
Acute cholecystitis refers to inflammation or infection of the gallbladder itself.
Symptoms commonly include:
- Severe RUQ pain
- Fever
- Tenderness beneath the ribs
- Persistent nausea
- Vomiting
- Symptoms lasting longer than 5–6 hours
Without treatment, infection may worsen rapidly.
Choledocholithiasis (Bile Duct Obstruction)
This occurs when a gallstone migrates into the common bile duct.
Because bile can no longer drain normally:
- Bilirubin accumulates
- Skin turns yellow
- Urine darkens
- Stools become pale
This blockage can become life-threatening if infection develops.
Gallstone Pancreatitis
A small stone may occasionally block the pancreatic drainage pathway.
Digestive enzymes become trapped and begin damaging the pancreas itself.
Symptoms may include:
- Severe upper abdominal pain
- Pain radiating into the back
- Sweating
- Vomiting
- Rapid worsening illness
Gallstone pancreatitis requires immediate hospital care.
Visual Recommendation: Flowchart showing progression from gallstones → bile duct obstruction → pancreatitis.
Outbound Reference Suggestions:
- American College of Gastroenterology (ACG)
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
- Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)
Risk Factors: Who Is Most Likely to Develop Gallstones?
Gallstones develop through a combination of:
- Hormonal influences
- Genetics
- Metabolic dysfunction
- Gallbladder motility changes
- Dietary factors
The “4 Fs” Risk Framework
Doctors sometimes summarize classic gallstone risk trends using the “4 Fs”:
- Female
- Forty
- Fertile
- Fat
This is not a rigid medical rule but rather a broad epidemiological pattern.
Female
Estrogen increases cholesterol concentration inside bile.
Forty
Risk generally rises with age.
Fertile
Pregnancy hormones slow gallbladder emptying.
Fat
Obesity increases cholesterol saturation and insulin resistance.
However, gallstones can still occur in younger adults, men, and individuals with normal body weight.
Intermittent Fasting and the “Gallbladder Freeze” Mechanism
Intermittent fasting itself does not automatically cause gallstones in healthy individuals.
However, prolonged fasting combined with extremely low fat intake may reduce gallbladder contractions significantly in susceptible patients.
Clinical Observation
Clinical observations suggest that prolonged fasting without sufficient dietary fat may limit release of CCK, resulting in bile stagnation, especially in individuals who already have sludge or pre-existing stones.
Without regular gallbladder emptying:
- Bile sits stagnant longer
- Cholesterol crystals accumulate
- Sludge thickens
- Stones form more easily
Some specialists informally refer to this process as the “Gallbladder Freeze” mechanism.”
Important Safety Recommendation
Individuals with a history of:
- Biliary sludge
- Gallstones
- Gallbladder attacks
- Rapid weight loss
should consult a healthcare professional before beginning aggressive fasting programs or extreme calorie restriction.
Moderate healthy fats such as:
- Olive oil
- Avocado
- Nuts
- Fatty fish
may help stimulate normal gallbladder contractions.
Rapid Weight Loss and Gallstones
Rapid weight loss significantly increases gallstone risk.
When body fat breaks down aggressively:
- The liver releases large amounts of cholesterol into bile
- Biliary sludge develops more easily
- Crystal formation accelerates
Clinical digestive guidelines commonly associate sustained weight loss exceeding approximately 1.5 kg (3.3 pounds) per week with increased gallstone formation risk in susceptible individuals.
This phenomenon is commonly observed after:
- Crash diets
- Ultra-low-calorie diets
- Bariatric surgery
- Severe illness
How Gallstones Are Diagnosed
Diagnosis usually begins with:
- Medical history
- Physical examination
- Symptom timeline
- Imaging tests
Ultrasound: The Gold Standard
Ultrasound remains the first-line imaging tool for gallstones because it is:
- Fast
- Non-invasive
- Widely available
- Highly effective
Gallstones appear as dense structures producing an acoustic shadow, a dark region behind the stone where sound waves cannot pass.
However, tiny stones or sludge may occasionally be missed.
HIDA Scan
A HIDA scan evaluates gallbladder function rather than simply detecting stones.
This test is particularly useful for suspected:
- Biliary dyskinesia
- Gallbladder hypomotility
- Functional gallbladder disorders
Biliary dyskinesia refers to gallbladder dysfunction without obvious stones. In these cases, the gallbladder may fail to empty properly despite normal ultrasound findings.
ERCP
ERCP (Endoscopic Retrograde Cholangiopancreatography) is both a diagnostic and therapeutic procedure.
It may be used when doctors suspect stones trapped inside the bile ducts.
Unlike ultrasound, ERCP can physically remove obstructing stones during the procedure.
Modern Treatment Strategies
Treatment depends on:
- Symptom severity
- Stone location
- Presence of infection
- Risk of recurrence
- Overall patient health
Watchful Waiting for Silent Gallstones
Silent gallstones often require no immediate intervention.
Doctors may recommend monitoring if:
- No pain exists
- No obstruction exists
- No inflammation exists
- Risk of complications remains low
Laparoscopic Cholecystectomy: The Gold Standard
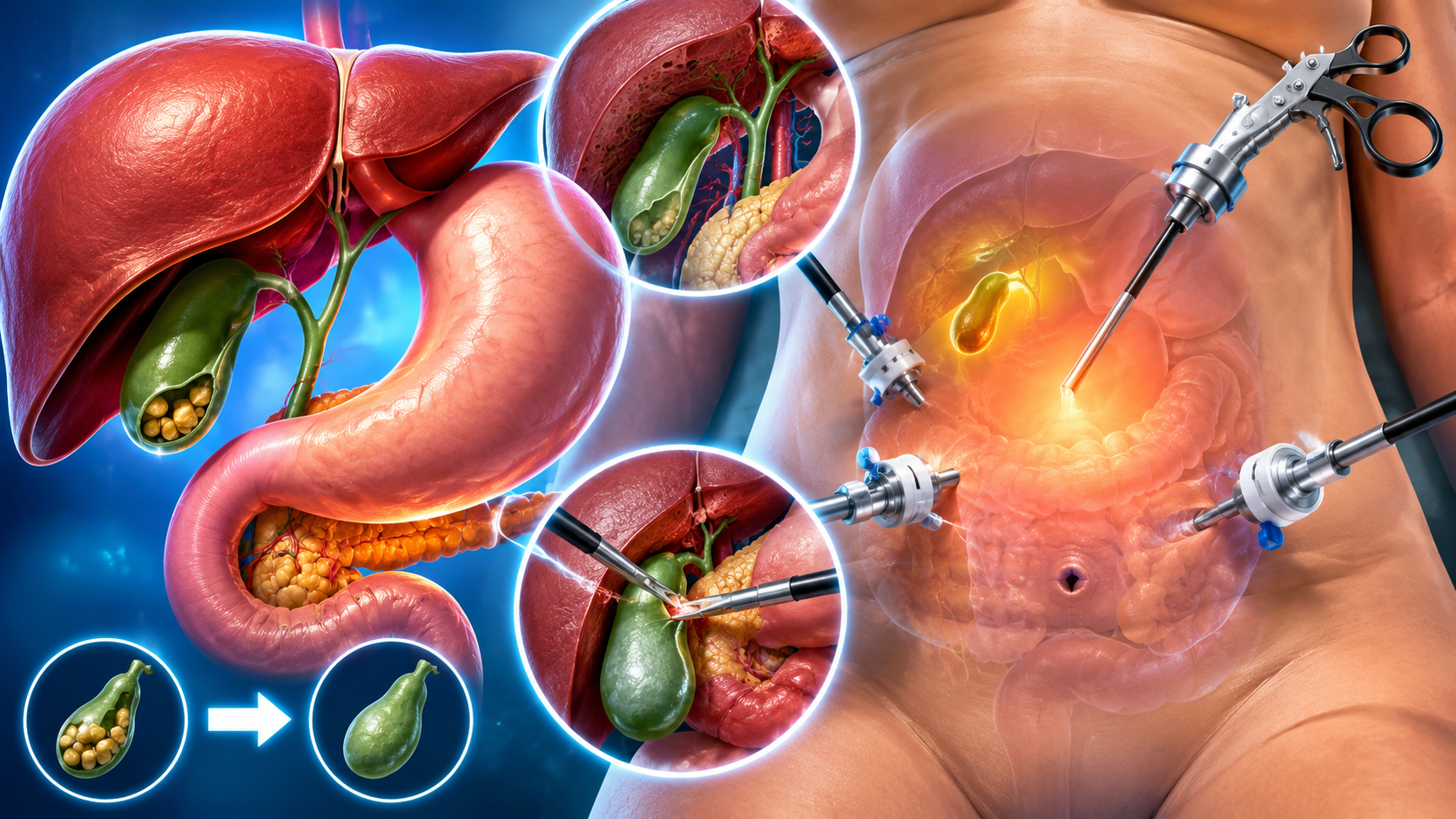
For symptomatic gallstones, the standard treatment is usually laparoscopic cholecystectomy, also called gallbladder removal surgery.
Modern laparoscopic surgery uses several small incisions instead of one large open incision.
Benefits commonly include:
- Faster recovery
- Smaller scars
- Reduced postoperative pain
- Shorter hospital stays
Many patients return to normal activity within 1–2 weeks depending on recovery progress.
Visual Recommendation: Illustration showing the minimally invasive laparoscopic approach.
Living Without a Gallbladder
Many patients fear digestion will stop functioning normally after gallbladder removal.
In reality:
- The liver continues producing bile
- Most patients adapt well over time
- Symptoms often improve dramatically once attacks stop
Some individuals experience temporary digestive sensitivity after surgery, especially following heavy meals.
Non-Surgical Treatment Options
Doctors sometimes prescribe ursodeoxycholic acid (Ursodiol) to dissolve certain cholesterol stones.
However, this treatment has important limitations.
Ursodiol generally works best only for:
- Small cholesterol stones
- Non-calcified stones
- Stones typically smaller than 10 mm
Treatment may require:
- Months to years
- Ongoing monitoring
- Long-term medication adherence
Even when successful, recurrence remains common after therapy stops.
Because gallbladder dysfunction often persists, surgery usually remains the more definitive long-term solution for symptomatic disease.
Self-Triage Checklist: When Should You Seek Care?
| Symptom | Urgency Level | Recommended Action |
| Mild intermittent bloating after meals | Low | Schedule routine medical evaluation |
| Recurrent RUQ pain after fatty foods | Moderate | Arrange outpatient assessment |
| Pain radiating to shoulder/back | Moderate | Seek prompt medical review |
| Pain lasting >5 hours | High | Go to the emergency room |
| Fever or jaundice | Emergency | Immediate emergency evaluation |
| Chest pressure with sweating or breathlessness | Emergency | Treat as potential cardiac emergency |
Frequently Asked Questions (FAQ)
Do all gallstones need to be removed?
No. Silent gallstones that do not cause symptoms or complications are often managed conservatively with observation.
Can gallstones dissolve without surgery?
Some small cholesterol stones may partially dissolve with Ursodiol, but treatment is slow and recurrence is common.
Why do gallbladder attacks happen after fatty meals?
Fat triggers release of cholecystokinin (CCK), which causes the gallbladder to contract forcefully. If a stone blocks bile flow during contraction, painful pressure develops.
Can gallstones cause symptoms without severe pain?
Yes. Some patients mainly experience bloating, nausea, excessive burping, or food intolerance before developing classic biliary colic.
Why does gallbladder pain radiate into the shoulder?
Gallbladder inflammation irritates the phrenic nerve near the diaphragm, causing referred pain that the brain perceives in the shoulder or upper back.
Conclusion
Gallstones can range from silent digestive findings to dangerous emergencies involving infection, pancreatitis, and bile duct obstruction.
Because gallbladder symptoms frequently imitate:
- Acid reflux
- Gastritis
- Muscle strain
- Indigestion
- Even heart attacks
many patients delay appropriate medical evaluation.
Understanding:
- What gallbladder pain feels like
- Why symptoms often occur after fatty meals
- Why pain radiates into the shoulder blade
- Which warning signs signal danger
- When emergency care becomes necessary
may help patients seek medical attention before complications become severe.
Persistent abdominal pain, jaundice, vomiting, fever, chest pressure, or breathing difficulty should always be evaluated by a qualified healthcare professional rather than self-diagnosed online.