Hashimoto Thyroiditis: Your Complete Roadmap to Diagnosis, Treatment, and Thriving
Your Hashimoto Thyroiditis Diagnosis: The Beginning of Understanding, Not the End of Well-Being
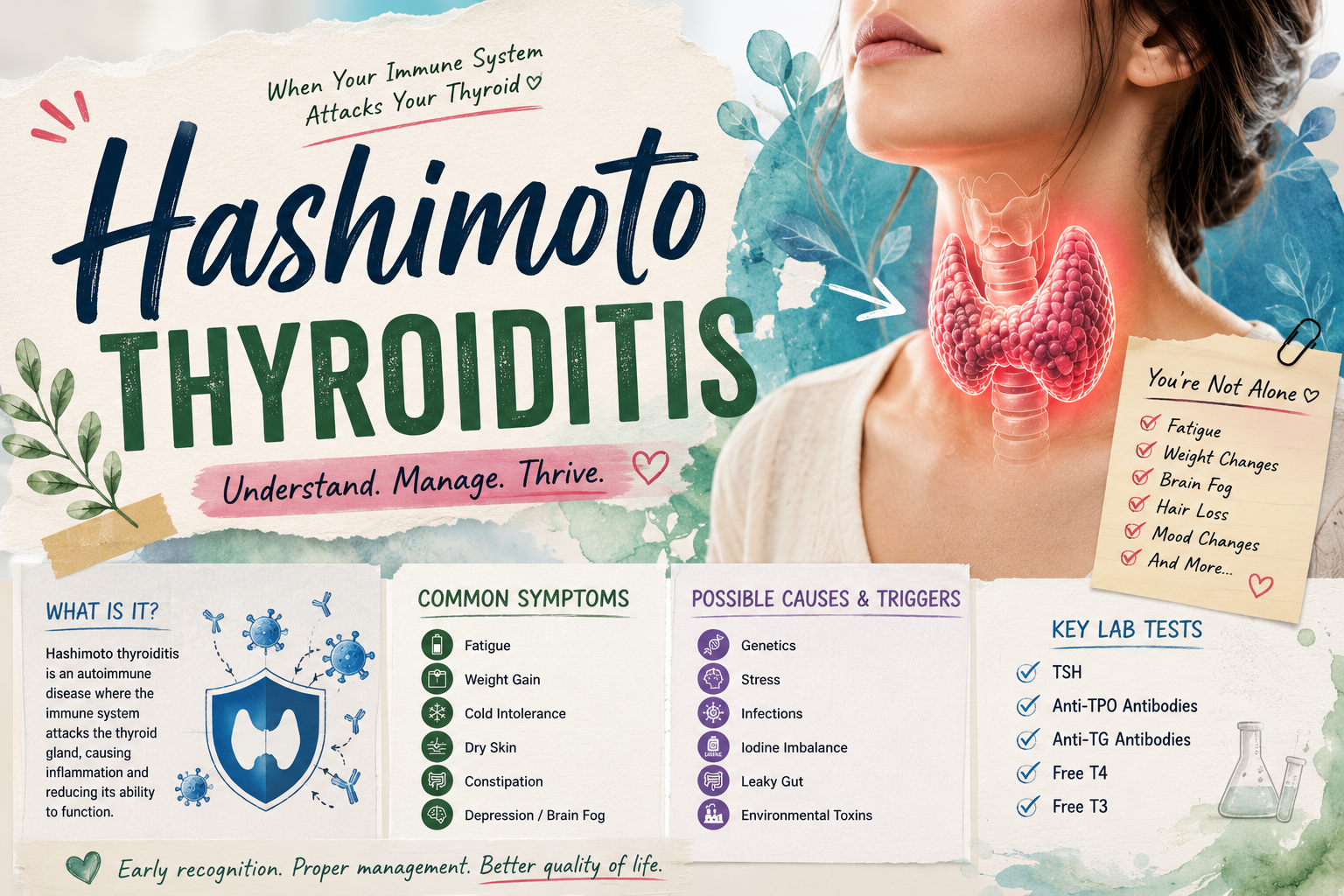
Receiving a diagnosis of Hashimoto thyroiditis can be a deeply disorienting experience. For many patients, it comes after months or even years of unexplained symptoms — fatigue that doesn't respond to rest, weight changes that defy dietary efforts, cognitive difficulties that make them question their own minds. In some ways, the diagnosis brings relief: finally, there is a name for what has been happening. In other ways, it raises a flood of questions, fears, and uncertainties about what life will look like going forward.
This guide is designed to be your comprehensive roadmap through Hashimoto thyroiditis — covering not just the clinical basics, but the nuanced realities of living with this condition day to day. From understanding what is happening in your body, to navigating the healthcare system, to making evidence-informed choices about nutrition, supplementation, and lifestyle, this article offers practical, actionable knowledge grounded in the best available science.
The Pathophysiology of Hashimoto Thyroiditis: A Detailed Look
Hashimoto thyroiditis is classified as a chronic lymphocytic thyroiditis — a condition in which lymphocytes (white blood cells) infiltrate and progressively destroy thyroid tissue. The process is initiated by autoreactive CD4+ T helper cells that inappropriately recognize thyroid antigens as foreign. Once activated, these T cells orchestrate a multi-pronged immune attack: they directly damage thyroid cells through cytotoxic mechanisms, they recruit B lymphocytes to produce autoantibodies, and they generate inflammatory cytokines (including TNF-alpha, IL-1, and interferon-gamma) that create a hostile local environment within the gland.
The characteristic histological appearance of Hashimoto thyroiditis — described by Hakaru Hashimoto himself in 1912 — includes dense lymphocytic infiltration, germinal center formation within the thyroid (a finding unique among thyroid conditions), destruction and replacement of normal follicular cells, and the accumulation of abnormal, enlarged cells called Hürthle cells (also known as oncocytes or oxyphilic cells). These histological features, visible on fine-needle aspiration biopsy or surgical specimens, remain the gold standard for definitive diagnosis when antibody testing and imaging are inconclusive.
The autoantibodies produced in Hashimoto thyroiditis — anti-TPO and anti-thyroglobulin — serve both as markers of the disease and as amplifiers of the inflammatory process. Anti-TPO antibodies, when bound to their target enzyme on thyroid cell membranes, activate the complement cascade, a destructive immune amplification system that punches holes in cell membranes. They also facilitate antibody-dependent cellular cytotoxicity (ADCC), in which natural killer cells use the antibodies as guidance systems to identify and destroy thyroid cells. This mechanism accelerates the destruction of remaining thyroid tissue, hastening progression to hypothyroidism.
Interpreting Your Lab Results: What the Numbers Mean
Understanding your own lab results is empowering and can significantly improve the quality of your conversations with your healthcare provider. Here is a guide to the key tests used in monitoring Hashimoto thyroiditis.
TSH (Thyroid-Stimulating Hormone): Produced by the pituitary gland, TSH is the most sensitive indicator of thyroid status. The conventional normal range is typically 0.5–4.5 mIU/L, though some endocrinologists advocate for a narrower therapeutic range of 1.0–2.5 mIU/L for people on treatment or those with symptoms. Elevated TSH indicates hypothyroidism (the pituitary is working harder to stimulate an underperforming thyroid). Suppressed TSH indicates hyperthyroidism or over-treatment.
Free T4 (fT4): This measures the level of unbound, biologically active thyroxine in the blood. It is a direct measure of thyroid hormone output. Normal range is typically 0.8–1.8 ng/dL (though lab ranges vary). Low fT4 with high TSH = overt hypothyroidism. Normal fT4 with high TSH = subclinical hypothyroidism.
Free T3 (fT3): Triiodothyronine is the biologically more active thyroid hormone, converted largely from T4 in peripheral tissues. Some patients with Hashimoto's have suboptimal T3 levels despite normal T4, which may explain persistent symptoms. Normal range is approximately 2.3–4.2 pg/mL. Testing fT3 is particularly valuable in patients with ongoing symptoms despite normalized TSH and T4.
Anti-TPO Antibodies: Normal is less than 35 IU/mL in most labs. Elevations confirm autoimmune thyroiditis. The absolute level does not reliably predict disease severity or progression rate. However, the trend over time — and whether levels change with treatment interventions — can be informative.
Anti-thyroglobulin Antibodies: Elevated in approximately 60–80% of Hashimoto's cases. Particularly useful in patients who are anti-TPO negative (seronegative Hashimoto's, which exists but is less common). The clinical interpretation is similar to anti-TPO antibodies.
The Treatment Spectrum: From Watchful Waiting to Comprehensive Management
Treatment decisions in Hashimoto thyroiditis should be individualized based on several factors: thyroid function (normal, subclinical, or overt hypothyroidism), symptom burden, pregnancy status, cardiovascular risk, bone density concerns, and patient preferences. A one-size-fits-all approach is inappropriate for a disease this heterogeneous.
Euthyroid Hashimoto's (normal TSH, positive antibodies): In the absence of symptoms and with normal thyroid function, many guidelines recommend watchful waiting with annual thyroid function monitoring. However, this should not mean abandoning the patient — lifestyle modifications, nutrient optimization, and strategies to reduce antibody levels are still relevant and appropriate.
Subclinical hypothyroidism (TSH 4.5–10 mIU/L): Treatment decisions depend on symptoms, age, cardiovascular risk, and whether the patient is pregnant or trying to conceive. Treatment is generally recommended for younger symptomatic patients, those with cardiovascular risk factors, and all pregnant women or those planning pregnancy. For older, asymptomatic patients with TSH below 7–8 mIU/L, monitoring may be appropriate.
Overt hypothyroidism (TSH >10 mIU/L, low fT4): Levothyroxine replacement is the standard of care. Starting dose is typically weight-based (approximately 1.6 mcg/kg/day), though elderly patients and those with cardiovascular disease start lower (25 mcg/day) and titrate gradually. TSH should be re-checked 6–8 weeks after any dose change.
Optimization beyond TSH normalization: Many patients on levothyroxine continue to have symptoms despite normal TSH. In these cases, it is worth evaluating fT3 levels, considering whether the addition of low-dose liothyronine (T3) might be beneficial, assessing for nutritional deficiencies that may impair thyroid function or worsen symptoms, and evaluating for co-existing conditions (such as adrenal insufficiency, anemia, or sleep apnea) that can mimic hypothyroid symptoms.
Nutrition as Medicine: Dietary Approaches Supported by Evidence
The role of nutrition in Hashimoto thyroiditis has attracted intense interest from both researchers and patients, and while definitive randomized controlled trial evidence remains limited in some areas, the cumulative body of evidence supports several dietary principles.
An anti-inflammatory dietary pattern — one that emphasizes whole foods, minimizes processed foods and added sugars, and provides ample anti-oxidants — is consistently associated with lower inflammatory markers and improved autoimmune disease activity. The Mediterranean diet, with its emphasis on vegetables, fruits, legumes, whole grains, fish, and olive oil, represents a well-studied template with extensive evidence for anti-inflammatory and cardioprotective effects.
Selenium is perhaps the most evidence-supported specific nutrient in Hashimoto thyroiditis management. Multiple randomized controlled trials have demonstrated that selenium supplementation at 200 mcg/day significantly reduces anti-TPO antibody titers, reduces inflammatory markers within the thyroid, and improves subjective well-being. Brazil nuts are a rich natural source (1–2 nuts per day can provide adequate selenium), though consistency of selenium content in nuts varies significantly with soil conditions. Selenium supplements (as selenomethionine) offer more reliable dosing.
The question of gluten in Hashimoto thyroiditis is nuanced. There is a well-established co-association between Hashimoto's and celiac disease, with studies finding celiac disease in approximately 4–6% of Hashimoto's patients — significantly above the general population prevalence of approximately 1%. For this subset of patients, strict gluten elimination is medically necessary and has been shown to reduce thyroid antibody levels. For the majority without celiac disease, the evidence for gluten elimination is less clear, but some patients report subjective improvement. A trial period of strict gluten elimination for 3–6 months, with objective re-assessment of antibodies and symptoms, is a reasonable personalized experiment.

Managing Hashimoto Flares: Recognizing and Responding to Disease Activity
Many people with Hashimoto thyroiditis describe periods of increased symptoms — fatigue, brain fog, joint pain, mood changes — that they identify as "flares." While the concept of flares is well-established in other autoimmune diseases, it is less formally recognized in Hashimoto's within conventional medicine, partly because flares don't always produce measurable changes in standard lab values.
Common triggers reported by Hashimoto's patients include significant psychological stress, acute illness (particularly viral infections), major hormonal changes (such as childbirth or menopause), dietary indiscretions (especially for those sensitive to gluten), sleep deprivation, and overexertion. Many patients find that identifying and managing their personal triggers is one of the most effective strategies for maintaining stability.
When a flare is suspected, practical responses include: prioritizing sleep and rest, temporarily reducing exercise intensity, increasing anti-inflammatory food consumption and reducing sugar and processed foods, checking thyroid function labs to assess whether medication adjustment is needed, addressing any identifiable stressors, and practicing stress-reduction techniques. Some patients have found short-term supplement interventions helpful during flares, including increased selenium, omega-3 fatty acids, and vitamin D, though these should be discussed with a healthcare provider.
Protecting Long-Term Health: Monitoring and Prevention of Complications
People with Hashimoto thyroiditis face several specific long-term health considerations that warrant proactive monitoring. Bone health is a concern, particularly for women, as both thyroid hormone excess (over-replacement) and thyroid hormone deficiency are associated with reduced bone mineral density. Maintaining thyroid levels within the optimal range and ensuring adequate calcium and vitamin D intake are important protective measures.
Cardiovascular health is another key consideration. Hypothyroidism is associated with dyslipidemia (particularly elevated LDL cholesterol), elevated blood pressure, and increased cardiovascular risk. These metabolic abnormalities are largely reversible with adequate thyroid hormone treatment, making consistent monitoring and treatment adherence critical.
The risk of thyroid lymphoma, while low in absolute terms, is approximately 67 times higher in Hashimoto's patients than in the general population. This underscores the importance of prompt evaluation of any rapidly enlarging thyroid gland, new or changing nodules, or symptoms suggesting compression of the neck structures (difficulty swallowing, hoarseness, or sensation of pressure in the throat).
Building Your Hashimoto Support Team
Managing Hashimoto thyroiditis effectively requires a team approach. Your primary care physician or endocrinologist provides the medical foundation of diagnosis and treatment. But optimizing outcomes in a complex, multisystem condition like Hashimoto's often benefits from additional expertise.
A registered dietitian with experience in autoimmune conditions can provide personalized guidance on dietary modifications and supplementation that is both evidence-based and practical. A mental health professional — particularly one familiar with chronic illness — can provide invaluable support for the psychological dimensions of living with Hashimoto's. A physical therapist or personal trainer with knowledge of autoimmune conditions can help design an exercise program that supports health without triggering flares.
Beyond the formal healthcare team, the peer support dimension of managing Hashimoto's should not be underestimated. Patient advocacy organizations, online communities, and local support groups provide a wealth of experiential knowledge, practical coping strategies, and — perhaps most importantly — the profound validation of knowing that others understand your experience. Hashimoto thyroiditis is a lifelong condition, but it is one that millions of people around the world are successfully managing, thriving with, and even using as a catalyst for deeper engagement with their own health and well-being. You do not have to face it alone.