Hashimoto's Disease Symptoms in Females: The Complete Gender-Specific Guide
Why Hashimoto's Disease Hits Women So Hard
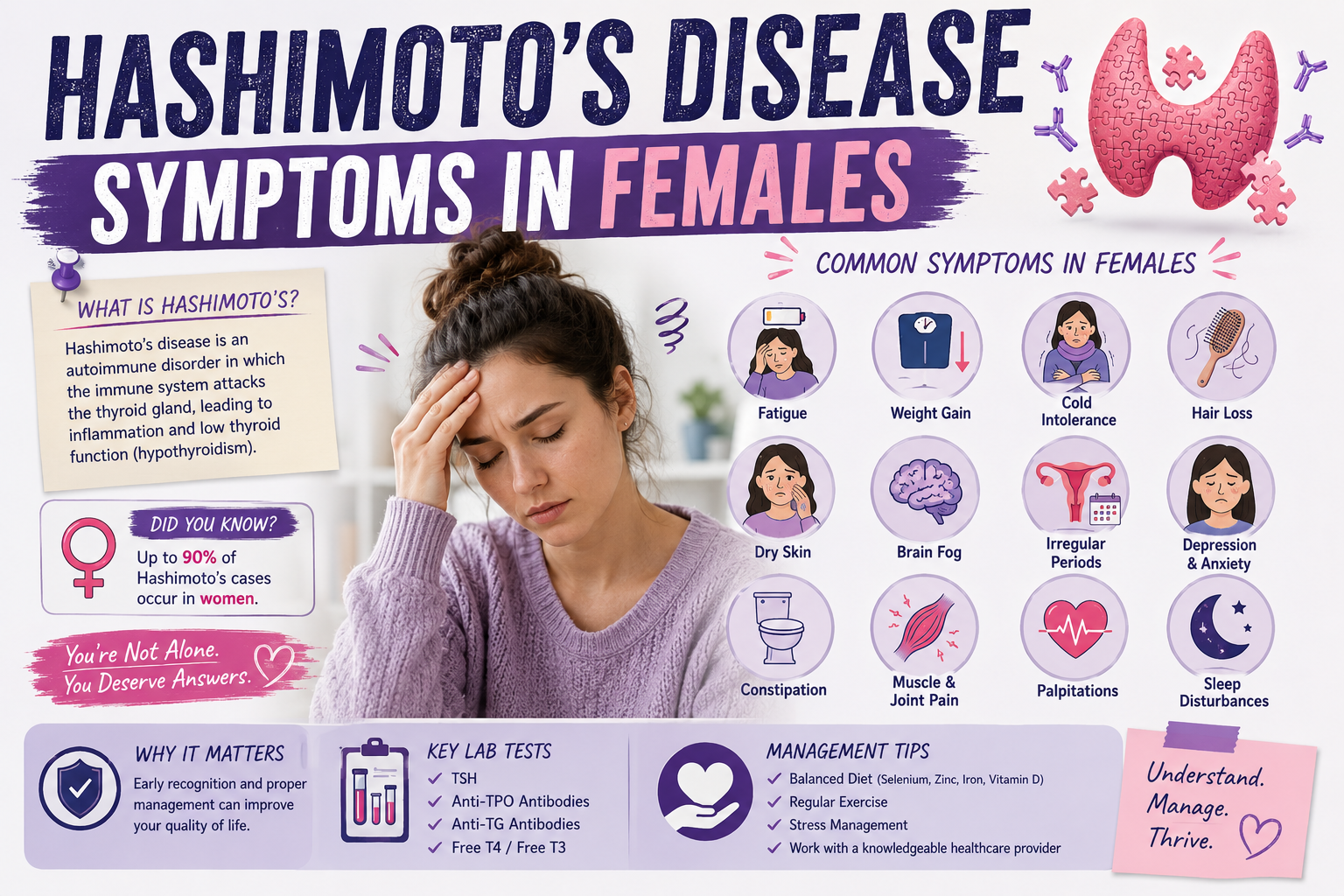
Of all the striking facts about Hashimoto's disease, perhaps none is more striking than this: women are diagnosed with the condition approximately seven to ten times more frequently than men. This is not a statistical quirk — it reflects a deep biological reality about the intersection of female sex hormones and immune regulation. Understanding this intersection is not only scientifically important; it is deeply practical for the millions of women navigating this condition through puberty, pregnancies, postpartum periods, perimenopause, and beyond.
But the female predominance of Hashimoto's also carries a troubling shadow. Because many of the symptoms of Hashimoto's disease overlap with conditions historically dismissed or minimized in female patients — fatigue attributed to "just stress," weight gain ascribed to poor habits, mood changes labeled as anxiety or depression — women with Hashimoto's often face years of being told their suffering is normal or psychosomatic before receiving an accurate diagnosis. This guide is dedicated to changing that: by naming and explaining every significant symptom that women with Hashimoto's disease experience, placing them in the context of female physiology, and providing a roadmap toward comprehensive care.
The Foundational Symptoms: What Hashimoto's Does to Energy, Weight, and Temperature
The most universally reported symptom cluster in Hashimoto's disease involves three closely related phenomena: profound fatigue, weight changes, and temperature dysregulation. Together, these three symptoms reflect the metabolic slowdown that results from inadequate thyroid hormone.
Fatigue: This is not the ordinary tiredness that follows a poor night's sleep or a demanding week. Hashimoto's fatigue is a pervasive, bone-deep exhaustion that persists regardless of how much rest is obtained. Women describe waking up already tired, struggling to get through the day on caffeine and willpower, and being unable to summon energy for activities they used to enjoy. The fatigue has a physical dimension — muscles feeling heavy and weak — and a cognitive one — the brain feeling slow and foggy. For many women, fatigue is the symptom that first prompted them to seek medical attention, and for many, it is the last to resolve even with treatment.
Weight gain: Unexplained weight gain — or difficulty losing weight despite dietary effort — is among the most distressing Hashimoto's symptoms for many women. The thyroid hormone-mediated slowdown in metabolic rate means the body burns fewer calories at rest. Fat accumulation tends to be generalized but may be particularly noticeable around the abdomen, face, and under the chin. Water retention contributes to puffiness, particularly around the eyes and face. Critically, this weight gain is not a character flaw or a failure of willpower — it is a physiological consequence of hormonal insufficiency, and it deserves to be addressed as such.
Cold intolerance: Feeling cold when others are comfortable, having cold hands and feet that never warm up, needing more clothing layers than everyone else in the room — these are hallmarks of hypothyroidism. Because thyroid hormones play a central role in thermogenesis (heat production), their deficiency compromises the body's ability to maintain temperature homeostasis. Women with Hashimoto's often find their cold intolerance to be one of the most pervasive quality-of-life impairments, affecting their comfort at work, their sleep quality, and their enjoyment of everyday activities.

Brain and Mood Symptoms: The Cognitive and Emotional Toll
Hashimoto's disease has profound effects on the brain, and many of the cognitive and emotional symptoms women experience are among the most debilitating — and the most frequently dismissed by clinicians who focus exclusively on thyroid hormone numbers.
Brain fog: "Brain fog" is the colloquial term for a constellation of cognitive symptoms that includes difficulty concentrating, impaired short-term memory, slowed mental processing, word-finding difficulties, and a pervasive sense of mental haziness. Women with Hashimoto's describe feeling like they are "operating through cotton wool," unable to think as clearly or quickly as they used to. In professional contexts, brain fog can impair job performance, creating additional stress and self-doubt. In social contexts, forgetting names, losing track of conversations, or struggling to articulate thoughts can be humiliating and isolating.
Depression: Rates of clinical depression are significantly elevated in women with Hashimoto's. Thyroid hormones directly modulate serotonergic, dopaminergic, and noradrenergic neurotransmitter systems — the very systems targeted by antidepressant medications. When thyroid hormone levels are suboptimal, the neurochemical environment of the brain shifts in ways that promote depressive symptoms. Many women with Hashimoto's have been prescribed antidepressants without adequate thyroid evaluation, receiving symptomatic treatment for what is, in part, a thyroid problem. This is not to say antidepressants are never appropriate — they may be needed — but addressing the thyroid component is essential.
Anxiety: Paradoxically, anxiety is also common in Hashimoto's, particularly in the earlier phases when transient hyperthyroid episodes (Hashitoxicosis) can create classic anxiety symptoms including racing heart, trembling, and a sense of impending doom. But anxiety also occurs in the hypothyroid phase, possibly related to the systemic inflammatory state, adrenal dysregulation, or the psychological burden of chronic illness.
Mood swings and emotional lability: Many women with Hashimoto's describe pronounced emotional lability — rapid mood shifts, increased emotional reactivity, difficulty managing frustration and irritability. These symptoms are particularly disruptive in the context of relationships and parenting, and they carry a significant burden of guilt and shame for women who feel they are "not themselves."
Skin, Hair, and Nails: The Visible Symptoms
The skin, hair, and nails are highly sensitive to thyroid hormone status, and their condition can provide important clues to the presence and severity of Hashimoto's hypothyroidism.
Hair loss and thinning: Hair loss is one of the most emotionally distressing symptoms for women with Hashimoto's. Because hair's cultural and personal significance for women is profound, hair thinning or loss can profoundly affect self-image and confidence. In hypothyroidism, hair loss typically presents as diffuse thinning of scalp hair rather than patchy loss (as in alopecia areata, a separate autoimmune condition). Hair may also become dry, coarse, and brittle. Eyebrow thinning — particularly the outer third of the eyebrows — is a classic but often overlooked sign of hypothyroidism that clinicians should actively seek. With adequate thyroid hormone treatment, hair loss typically improves, though full regrowth can take many months.
Dry, rough skin: Reduced sweating and decreased skin cell turnover in hypothyroidism produce characteristically dry, rough, and sometimes scaly skin. The skin may feel coarser to the touch, and fine lines may appear more prominent. Wound healing may be impaired. The face, particularly around the eyes and on the cheeks, may appear puffy due to the accumulation of mucopolysaccharides in the dermis — a process called myxedema — that gives the face a characteristic fullness distinct from simple fluid retention.
Brittle nails: Nails become brittle, slow-growing, and may develop ridges or striations. They are more prone to breaking and peeling. This reflects the impact of thyroid hormone deficiency on keratinocyte proliferation and nail matrix function.
Menstrual and Reproductive Symptoms: The Female-Specific Dimension
The intersection of Hashimoto's disease with female reproductive physiology is one of the most distinctive and clinically important aspects of this condition in women. Thyroid hormones have extensive interactions with the hypothalamic-pituitary-ovarian (HPO) axis, and thyroid dysfunction can disrupt the menstrual cycle, fertility, and reproductive outcomes in multiple ways.
Menstrual irregularities: Hashimoto's hypothyroidism can cause a wide range of menstrual disturbances. Heavy, prolonged periods (menorrhagia) are among the most common, resulting from the effects of thyroid hormone deficiency on coagulation factors and uterine contractility. Some women experience more frequent periods; others may experience oligomenorrhea (infrequent periods) or amenorrhea (absence of periods) in severe hypothyroidism. Painful periods (dysmenorrhea) are also over-represented in Hashimoto's patients, possibly related to prostaglandin dysregulation.
Impaired fertility: Hypothyroidism, including subclinical hypothyroidism, is associated with reduced conception rates, increased risk of ovulation disorders (including polycystic ovary syndrome-like presentations), and elevated miscarriage risk. TSH levels should ideally be below 2.5 mIU/L prior to conception and maintained below 2.5 mIU/L throughout the first trimester to optimize fetal development. Women with Hashimoto's who are struggling to conceive should have comprehensive thyroid evaluation as a routine component of fertility workup.
Pregnancy complications: Women with Hashimoto's face elevated risks during pregnancy including miscarriage (particularly in the first trimester), preeclampsia, placental abruption, preterm birth, and gestational hypertension. The fetus depends entirely on maternal thyroid hormone for the first 10–12 weeks of development before its own thyroid gland begins functioning — making maternal thyroid status during early pregnancy critically important for fetal brain development. Inadequately treated hypothyroidism during pregnancy has been associated with lower IQ scores in offspring in several studies, though this risk is largely mitigated by appropriate treatment.
Postpartum thyroiditis: Women with Hashimoto's have significantly elevated rates of postpartum thyroiditis — a transient autoimmune thyroid condition that develops within the first year after delivery. It typically follows a triphasic course: a hyperthyroid phase (weeks 1–4 postpartum), a hypothyroid phase (months 4–8), and eventual recovery. Approximately 25–30% of women with postpartum thyroiditis who have pre-existing anti-TPO antibodies will develop permanent hypothyroidism within 5–10 years.

Hashimoto's Through the Life Stages of Women
In teenage girls: Adolescent-onset Hashimoto's deserves particular attention because its impact during this critical developmental period is substantial. Poorly controlled hypothyroidism in teenage girls can impair linear growth, delay pubertal development or cause menstrual irregularities from puberty's onset, impair academic performance, and contribute to mood disorders during an already emotionally turbulent period. Screening for thyroid antibodies should be considered in teenage girls with unexplained fatigue, weight changes, menstrual irregularities, or school performance decline.
In women with PCOS: Polycystic ovary syndrome (PCOS) and Hashimoto's disease show significant clinical overlap and may co-exist. Hashimoto's can contribute to insulin resistance, androgen excess, and menstrual irregularities that mimic or worsen PCOS. Conversely, the insulin resistance and chronic inflammation of PCOS may promote autoimmune activity. Women with PCOS should be routinely screened for thyroid antibodies, and women with Hashimoto's who present with features of androgen excess or polycystic ovaries warrant evaluation for PCOS.
In perimenopausal and menopausal women: The hormonal turbulence of perimenopause creates significant diagnostic complexity for women with Hashimoto's. Hot flashes, night sweats, weight gain, mood changes, sleep disruption, and cognitive symptoms occur in both conditions, making it difficult to attribute symptoms to one cause versus the other. Comprehensive evaluation is essential, and both conditions may require concurrent management. Declining estrogen levels in menopause may also affect thyroid hormone requirements — some women on levothyroxine find their dose needs adjustment after menopause.
Managing Hashimoto's Symptoms in Females: A Personalized Approach
Effective management of Hashimoto's disease in women requires a personalized, holistic approach that accounts for each woman's unique hormonal context, life stage, symptom profile, and personal priorities. The foundation remains thyroid hormone optimization — but "optimization" means more than simply achieving a TSH within the reference range. It means finding the thyroid hormone level at which a woman feels genuinely well, functions optimally, and experiences minimal symptom burden.
For many women, this requires thyroid hormone levels toward the lower end of the TSH range (1.0–2.0 mIU/L). For some, particularly those with persistently low fT3 on levothyroxine alone, combination therapy with T3 (as liothyronine or desiccated thyroid extract) may be transformative. Nutritional optimization — including adequate selenium, vitamin D, iron (which is often depleted in women with heavy periods), vitamin B12, and zinc — is critically important and should be addressed through both dietary improvements and targeted supplementation as indicated.
Stress management and sleep optimization are not optional lifestyle extras for women with Hashimoto's — they are therapeutic necessities. The strong bidirectional relationship between the stress response and immune regulation means that chronic stress actively perpetuates autoimmune disease activity. Finding sustainable stress reduction strategies — whether yoga, therapy, boundary-setting in professional and personal life, or community connection — is one of the most powerful long-term investments a woman with Hashimoto's can make in her own health.
Finally, advocacy matters. Women with Hashimoto's deserve to be listened to, believed, and thoroughly evaluated. They deserve providers who understand that symptoms can persist despite "normal" lab values, who consider the full hormonal context of the female life stage, and who partner with them in treatment decisions rather than dismissing their experience. Finding such a provider — whether an endocrinologist, functional medicine physician, or integrative health practitioner — can be one of the most important steps in a woman's Hashimoto's journey.