Hashimoto's: The Hidden Epidemic Affecting Millions and How to Fight Back
The Story of Hakaru Hashimoto and the Disease That Bears His Name
In 1912, a young Japanese physician named Hakaru Hashimoto published a landmark paper describing a condition he observed in four women — a novel form of thyroid disease characterized by lymphocytic infiltration of the gland, fibrosis, and a distinctive clinical picture he called "struma lymphomatosa." His paper, published in a German surgical journal, would go largely unrecognized for decades. It wasn't until the 1950s, nearly a half-century later, that the medical community fully recognized the condition as an autoimmune disease and named it Hashimoto's thyroiditis in his honor.
Today, Hashimoto's disease is recognized as the most common autoimmune disorder worldwide and the most frequent cause of hypothyroidism in developed countries. By some estimates, it affects between 5 and 10 percent of the global population, with women making up the overwhelming majority of those diagnosed. Yet despite its prevalence, Hashimoto's remains profoundly underdiagnosed — with some studies suggesting that for every person who knows they have it, multiple others are living with the condition unaware.
The Mechanics of Hashimoto's: How the Immune System Destroys the Thyroid
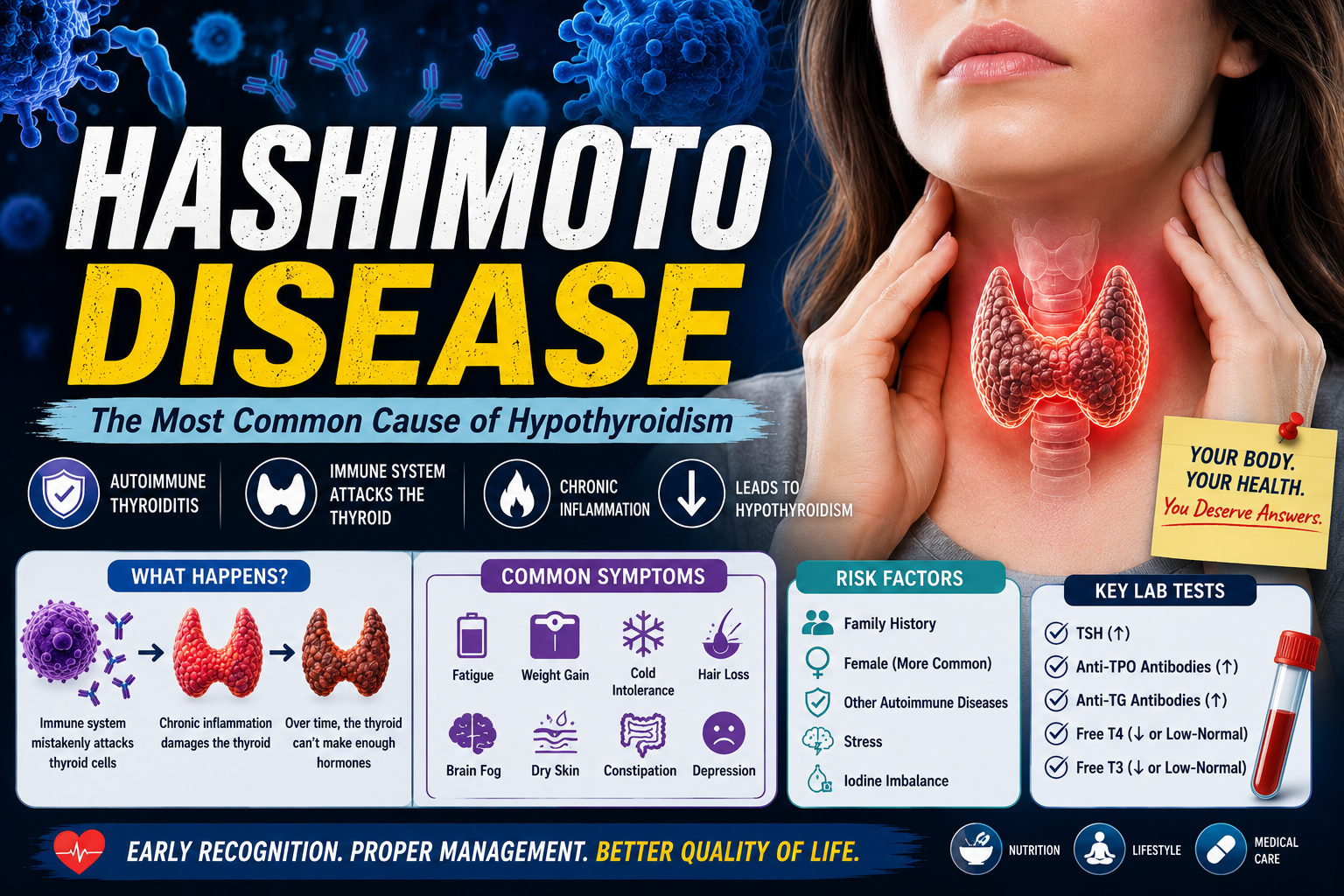
Hashimoto's disease begins with a failure of immune tolerance. Normally, the immune system is carefully trained to distinguish between the body's own proteins and foreign invaders. In Hashimoto's, this training fails, and the immune system begins producing antibodies and T lymphocytes that target two key thyroid proteins: thyroid peroxidase (TPO), which is essential for synthesizing thyroid hormone, and thyroglobulin (Tg), the precursor protein from which T3 and T4 are made.
These autoreactive immune cells infiltrate the thyroid tissue, creating a chronic inflammatory environment within the gland. Over time, the relentless immune assault destroys thyroid follicular cells (thyrocytes) — the working cells that produce thyroid hormone. The gland's ability to maintain adequate hormone production gradually diminishes. Initially, the pituitary compensates by releasing more TSH to drive whatever remaining thyroid capacity exists, but eventually the gland can no longer keep up, and frank hypothyroidism develops.
The speed of this progression is highly variable. Some individuals transition from normal thyroid function to overt hypothyroidism within a few years of diagnosis. Others have detectable antibodies for decades without ever developing significant hormonal abnormalities. This variability reflects the complex interplay of genetic, environmental, and hormonal factors that modulate disease activity in each individual.
The Hashimoto's Patient Experience: Beyond the Lab Results
One of the most challenging aspects of Hashimoto's disease — and one that healthcare providers sometimes underappreciate — is the profound gap between what laboratory tests show and how patients actually feel. Many people with Hashimoto's experience a wide range of symptoms that significantly impair their quality of life, even when their TSH level falls within the normal reference range.
This "normal labs, abnormal life" phenomenon is one of the most common complaints in Hashimoto's patient communities. The symptoms that define the lived experience of Hashimoto's extend far beyond the classic hypothyroid features. Fatigue is almost universally reported — but this is not ordinary tiredness. It is a bone-deep exhaustion that persists regardless of how much sleep is obtained, that makes even simple tasks feel monumentally difficult, and that is not relieved by caffeine or motivation alone.
Brain fog — a term that covers difficulty concentrating, memory lapses, word-finding problems, and a pervasive sense of mental cloudiness — is another defining feature. Patients describe feeling as if they are "thinking through cotton wool" or operating at a fraction of their normal cognitive capacity. This symptom, which has no established objective measure and is therefore frequently dismissed by clinicians, can be profoundly disabling and affects work performance, relationships, and self-esteem.
Mood disturbances — particularly depression and anxiety — are disproportionately common in Hashimoto's patients. Whether this represents a direct neurological effect of thyroid hormone insufficiency, a consequence of chronic illness burden, or a shared immunological pathway between thyroid autoimmunity and mood disorders remains an active research question. What is clear is that antidepressants alone, without addressing the underlying thyroid condition, are often inadequate.
Who Is at Risk? Understanding the Risk Profile for Hashimoto's
Several factors significantly increase a person's risk of developing Hashimoto's disease. Understanding these risk factors is important for early identification of at-risk individuals and for motivating proactive monitoring and lifestyle modifications.
Female sex: Women are 7–10 times more likely to develop Hashimoto's than men. Estrogen appears to promote autoimmunity in multiple ways, including by enhancing B-cell responses and antibody production. Testosterone, by contrast, appears to have immunosuppressive effects — which may partly explain the relative protection seen in men. The risk for women peaks in the childbearing years but remains elevated throughout life.
Family history: Having a first-degree relative with Hashimoto's, Graves' disease, or another autoimmune condition significantly elevates risk. Genetic variants in multiple immune-regulatory and thyroid-specific genes have been identified as risk factors. However, because genetics does not determine destiny in autoimmune disease, lifestyle and environmental factors remain critically important modifiable variables.
Pregnancy and postpartum period: The dramatic hormonal and immune shifts of pregnancy and the postpartum period create specific windows of vulnerability. Postpartum thyroiditis — which is immunologically related to Hashimoto's — affects approximately 5–10% of women and is a significant risk factor for the eventual development of permanent hypothyroidism. Women with pre-existing anti-TPO antibodies before pregnancy face a substantially elevated risk of postpartum thyroiditis and subsequent Hashimoto's.
Iodine status: Both iodine deficiency and iodine excess have been linked to increased Hashimoto's risk. This creates a nuanced situation with regard to iodine supplementation: while adequate iodine is necessary for thyroid function, excess iodine — which can occur with high-dose supplement use — may trigger or exacerbate autoimmune thyroid disease in susceptible individuals.
The Relationship Between Hashimoto's and Mental Health
The connection between Hashimoto's disease and mental health deserves special attention, as it remains underappreciated in clinical settings. Multiple lines of evidence support a bidirectional relationship between thyroid autoimmunity and psychiatric conditions. Elevated anti-TPO antibody levels have been found in a significant proportion of patients with depression, bipolar disorder, and postpartum depression — even in individuals whose thyroid function tests appear normal.
Research has suggested that thyroid antibodies may have direct neurological effects, potentially influencing serotonin, norepinephrine, and dopamine signaling in the brain. Some studies have found that psychiatric symptoms in Hashimoto's patients improve with thyroid hormone treatment even when TSH is technically within the normal range, suggesting that the brain may be more sensitive to thyroid hormone levels than the pituitary's feedback loop reveals.
Hashimoto's encephalopathy — a rare but serious condition characterized by neuropsychiatric symptoms, seizures, and cognitive deterioration in the setting of high anti-TPO antibodies — represents the extreme end of this brain-thyroid connection. While uncommon, it serves as a dramatic illustration of the potential neurological impact of thyroid autoimmunity.

Hashimoto's and Fertility: What Every Woman Should Know
For women of reproductive age, Hashimoto's disease has important implications for fertility and pregnancy outcomes. Even subclinical hypothyroidism — where TSH is mildly elevated but free T4 remains normal — is associated with increased risk of difficulty conceiving, miscarriage, premature birth, and impaired fetal neurodevelopment. Thyroid hormones are critically important for the development of the fetal brain, and the fetus depends entirely on maternal thyroid hormone supply for the first 10–12 weeks of pregnancy, before its own thyroid begins functioning.
Current guidelines recommend checking thyroid function in women who are trying to conceive or who have experienced recurrent miscarriage. Women with Hashimoto's who are planning pregnancy should discuss optimal preconception thyroid optimization with their physician. During pregnancy, thyroid hormone requirements typically increase by approximately 30–50%, meaning that women on levothyroxine replacement will often need dose adjustments as soon as pregnancy is confirmed.
The good news is that with appropriate monitoring and management, women with Hashimoto's can and do have successful pregnancies and healthy babies. The key is proactive communication with a healthcare team that includes appropriate thyroid surveillance throughout pregnancy and the postpartum period.
The Emerging Science of Hashimoto's: What Research Is Revealing
Scientific understanding of Hashimoto's disease is advancing rapidly. Several research areas are particularly exciting for their potential to transform diagnosis, treatment, and ultimately prevention of the condition.
Precision medicine approaches are beginning to move Hashimoto's management beyond the "one TSH fits all" paradigm. Research into individual genetic variants affecting T4-to-T3 conversion, thyroid hormone receptor sensitivity, and immune regulatory pathways is helping identify which patients are likely to benefit from specific treatment approaches, including combination T4/T3 therapy.
The microbiome-autoimmunity connection is another frontier with significant promise. Studies have found distinct gut microbiome alterations in Hashimoto's patients, and animal models suggest that microbiome manipulation can influence the development of autoimmune thyroid disease. Clinical trials of targeted probiotic interventions are underway. Meanwhile, the concept of intestinal permeability — colloquially "leaky gut" — as a facilitator of autoimmunity is gaining scientific credence, with evidence suggesting that a compromised gut barrier may allow luminal antigens to trigger systemic immune responses in genetically susceptible individuals.
Immunotherapy approaches, borrowed from the oncology field, are also being explored. The potential to reset dysregulated immune responses — either through tolerogenic vaccines, regulatory T cell therapy, or targeted cytokine modulation — represents an exciting long-term prospect for disease modification rather than mere symptom management.
Practical Daily Strategies for Managing Hashimoto's
While research continues to advance, people living with Hashimoto's today can meaningfully improve their quality of life through practical daily strategies. Medication adherence and consistent lab monitoring form the foundation. Levothyroxine should be taken consistently, ideally on an empty stomach 30–60 minutes before food, and away from supplements (especially calcium, iron, and magnesium) that can impair absorption.
Nutrition plays a significant role. An anti-inflammatory dietary pattern — emphasizing vegetables, fruits, fish, olive oil, and legumes while minimizing ultra-processed foods, refined sugars, and trans fats — reduces systemic inflammation and may help modulate antibody activity. Ensuring adequate selenium, zinc, vitamin D, and iron status is important, as deficiencies in these nutrients are common in Hashimoto's and can worsen symptoms. Regular, moderate physical activity is beneficial, though intensity should be calibrated to current health status.
Community and psychological support are often undervalued but critically important components of long-term well-being with Hashimoto's. The chronic, fluctuating nature of the disease — combined with the frustration of often being dismissed within the healthcare system — can take a significant psychological toll. Connecting with others who understand the lived experience of Hashimoto's, whether through patient support groups, online communities, or patient advocacy organizations, can provide both practical information and the profound comfort of being truly understood.