Rotator Cuff: Complete Guide to Anatomy, Injuries, Treatment, and Recovery
What Is the Rotator Cuff? Understanding the Anatomy
The rotator cuff is a group of four muscles and their associated tendons that surround the shoulder joint, forming a protective "cuff" around the head of the upper arm bone (humerus). These muscles originate from the scapula (shoulder blade) and insert into the greater and lesser tubercles of the humerus, holding the ball of the shoulder joint firmly within the shallow socket of the scapula (the glenoid). Without the rotator cuff, the shoulder — which has the greatest range of motion of any joint in the body — would be dangerously unstable.
The Four Muscles of the Rotator Cuff
The supraspinatus is the most commonly injured rotator cuff muscle. It runs along the top of the shoulder blade and is responsible for lifting the arm away from the body (abduction), particularly the first 15 degrees of movement. Because of its position beneath the acromion — a bony projection of the scapula — the supraspinatus tendon is especially vulnerable to impingement and tear.
The infraspinatus is a large, triangular muscle located in the infraspinous fossa of the scapula. Together with the teres minor, it handles external rotation of the arm, which is the motion of rotating the arm outward away from the body. Strong infraspinatus function is critical for overhead athletes, including pitchers, swimmers, and tennis players.
Several specific physical examination tests have been developed to assess the integrity of the rotator cuff and help identify which tendons are involved. The Neer impingement sign involves passive forward elevation of the arm to compress the supraspinatus tendon under the acromion. The Hawkins-Kennedy test reproduces impingement by internally rotating the arm at 90 degrees of flexion. The drop arm test assesses supraspinatus integrity by asking the patient to slowly lower a fully abducted arm. The lift-off test evaluates subscapularis function by having the patient lift the hand away from the lower back against resistance. The external rotation lag sign is used to detect large or massive posterior superior rotator cuff tears. Each of these tests has different sensitivity and specificity, and no single test is sufficient on its own to diagnose a rotator cuff tear definitively.
Imaging Studies for Rotator Cuff Diagnosis
X-rays (plain radiographs) are usually the first imaging modality ordered, primarily to rule out bony abnormalities such as fractures, arthritis, or acromial bone spurs. X-rays cannot directly visualize soft tissue injuries, however. Ultrasound is an increasingly popular diagnostic tool for rotator cuff evaluation due to its low cost, real-time dynamic assessment capability, and lack of radiation. A skilled musculoskeletal sonographer can detect both partial and full-thickness rotator cuff tears with diagnostic accuracy comparable to MRI. Magnetic Resonance Imaging (MRI) remains the gold standard for rotator cuff diagnosis, offering detailed visualization of the rotator cuff tendons, muscles, and surrounding structures. MRI can identify the exact location, size, and extent of a tear, as well as associated findings such as muscle atrophy and fatty infiltration, which are critical for surgical planning. MRI arthrography — in which contrast dye is injected into the shoulder joint before scanning — is particularly useful for detecting partial-thickness articular-side tears.
Rotator Cuff Treatment Options: From Conservative Care to Surgery
Treatment for rotator cuff injuries is not one-size-fits-all. The optimal approach depends on multiple factors, including the patient's age, activity level, the type and severity of the injury, the duration of symptoms, and their personal goals and expectations. For many patients, especially those with degenerative tears or mild to moderate partial tears, non-surgical treatment is highly effective. For others — particularly younger patients with acute full-thickness tears or those who have failed conservative management — surgery may be the best option.
Non-Surgical (Conservative) Treatment
Conservative treatment for rotator cuff injuries typically begins with rest and activity modification — avoiding the overhead activities and movements that aggravate symptoms. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, can help control pain and inflammation in the short term. Ice application for 15 to 20 minutes several times per day can also reduce swelling and discomfort, particularly in the acute phase of injury.
Physical therapy is the cornerstone of conservative rotator cuff treatment. A structured physical therapy program focuses on reducing pain and inflammation, restoring range of motion, and progressively strengthening the rotator cuff and surrounding shoulder muscles. Studies show that a well-designed physical therapy protocol can produce outcomes equivalent to surgery for many patients with full-thickness rotator cuff tears, particularly older and less active individuals. Corticosteroid injections into the subacromial space can provide substantial pain relief and improved function, especially when pain is the primary barrier to participation in physical therapy. However, repeated injections are generally avoided due to their potential to weaken tendon tissue and accelerate degeneration.
Surgical Treatment for Rotator Cuff Tears
When conservative treatment fails to relieve symptoms after three to six months, or when the injury is acute, large, or involves a high-demand patient, surgery is typically recommended. The most common surgical approach is arthroscopic rotator cuff repair, a minimally invasive procedure in which the surgeon uses a small camera (arthroscope) and specialized instruments inserted through tiny incisions to reattach the torn tendon to the bone using anchors. Arthroscopic repair has become the dominant surgical technique due to its lower complication rates, reduced post-operative pain, faster recovery, and excellent clinical outcomes compared to traditional open surgery.
In cases of irreparable massive rotator cuff tears, alternative surgical procedures may be considered. Superior capsule reconstruction (SCR) uses a graft — either from the patient's own tissue or from a donor — to restore superior shoulder stability. Reverse total shoulder arthroplasty (RTSA) is another option for patients with massive irreparable tears accompanied by significant arthritis or rotator cuff tear arthropathy, in which the joint surfaces are replaced with a prosthetic implant designed to allow shoulder function even without an intact rotator cuff.
Rotator Cuff Rehabilitation: Exercises and Recovery Timeline
Whether recovering from conservative treatment or post-surgical repair, rehabilitation is the most critical determinant of long-term rotator cuff outcomes. A well-structured rehabilitation program is not just about returning to prior activity levels — it is about rebuilding strength, coordination, and resilience in a shoulder that has been compromised by injury or surgery. Rehabilitation is typically divided into phases, each building on the progress of the previous one.
Phase 1: Protection and Pain Control (Weeks 1-6)
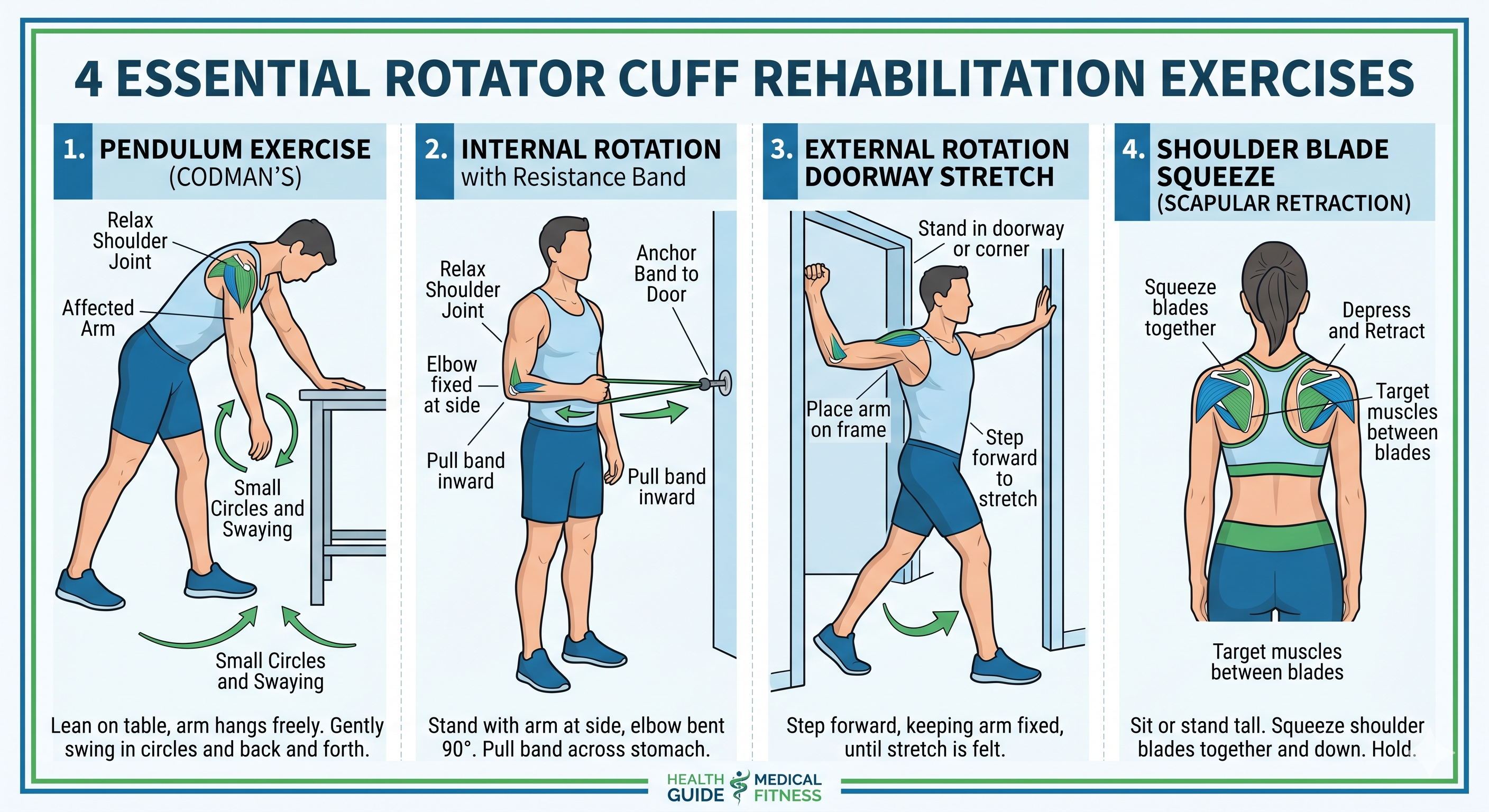
In the initial phase of recovery, the primary goals are to protect the healing tissue, control pain and swelling, and maintain mobility in the shoulder, elbow, wrist, and hand. Patients who have undergone surgical repair typically wear a sling for four to six weeks to protect the repaired tendon. Pendulum exercises — in which the patient bends forward and allows the arm to swing gently in circles using gravity — are one of the earliest exercises introduced and are valuable for maintaining glenohumeral joint mobility without stressing the repair. Passive and assisted range-of-motion exercises performed by a therapist or with the help of the other arm are gradually introduced as healing progresses.
Phase 2: Restoring Range of Motion (Weeks 6-12)
As healing progresses and pain decreases, the focus shifts to restoring full active range of motion. Active-assisted exercises using a pulley system or a cane are commonly employed to gradually recover elevation and rotation. Stretching exercises targeting the posterior capsule of the shoulder — such as the cross-body stretch and the sleeper stretch — help address the tightness that frequently develops following rotator cuff injury. Patient education on proper posture and scapular positioning is also critical during this phase, as poor scapular mechanics can significantly impede recovery and lead to persistent impingement.
Phase 3: Strengthening (Months 3-6)
Strengthening exercises are introduced progressively once adequate range of motion has been restored and pain is well controlled. Resistance band exercises are particularly effective for rotator cuff rehabilitation because they allow controlled, progressive loading across multiple planes of motion. Key strengthening exercises include internal and external rotation with a resistance band, side-lying external rotation, prone Y, T, and W exercises for scapular stabilizers, and side-lying forward flexion. It is essential to progress strengthening exercises gradually and under the guidance of a qualified physical therapist, as premature or excessive loading can compromise the repair or healing tissue.

Phase 4: Return to Activity (Months 6-12)
The final phase of rehabilitation focuses on sport-specific or work-specific training, functional movement patterns, and building the endurance and power required for the patient's desired activities. Return to full activity after rotator cuff repair is a gradual process that should be based on objective criteria — including strength testing, pain levels, and functional performance tests — rather than a fixed calendar timeline. Most patients who undergo arthroscopic rotator cuff repair can expect to return to light daily activities within 2-3 months, overhead sports within 9-12 months, and heavy labor or high-demand sports within 12-18 months.
How to Prevent Rotator Cuff Injuries
While not all rotator cuff injuries can be prevented, particularly those related to aging and genetics, there is strong evidence that targeted exercise programs can significantly reduce the risk of injury and re-injury. Prevention strategies are particularly important for athletes and workers in high-risk occupations.
Strengthening the rotator cuff muscles through a regular exercise program is the single most effective prevention strategy. A balanced shoulder strengthening program should include exercises for all four rotator cuff muscles, with particular emphasis on external rotation and scapular stabilization, as these are the muscle groups most commonly found to be weak in patients with shoulder problems. Strengthening the deltoid, biceps, and triceps is important as well, as these muscles work synergistically with the rotator cuff.
Proper technique and ergonomics are equally important. Athletes should work with qualified coaches to ensure that their throwing, swimming, or serving mechanics are biomechanically sound. Workers performing overhead tasks should receive ergonomics training and use appropriate tools and equipment to minimize subacromial stress. Regular stretching of the posterior shoulder capsule, warm-up routines before exercise, and adequate rest between training sessions are also key components of an effective injury prevention strategy.
Lifestyle modifications can also play a role in rotator cuff health. Smoking cessation is strongly recommended, as nicotine constricts the small blood vessels supplying the tendons and impairs the body's ability to repair micro-damage. Maintaining a healthy body weight reduces the overall load on the shoulder joint. Ensuring adequate intake of nutrients important for tendon health — including vitamin C, collagen precursors, and omega-3 fatty acids — may also provide some benefit, though the evidence base for nutritional interventions in tendon health is still developing.
When to See a Doctor for Shoulder and Rotator Cuff Pain
Many people make the mistake of dismissing shoulder pain or trying to "push through" it, only to find that what began as a minor rotator cuff problem has evolved into a major one. Early medical evaluation is important, particularly if you experience any of the following: sudden, severe shoulder pain following a fall or direct trauma; inability to raise the arm or severe arm weakness; persistent shoulder pain lasting longer than one to two weeks despite rest and over-the-counter pain medication; significant nighttime pain that disrupts sleep; a visible deformity or swelling in the shoulder; or shoulder pain accompanied by other symptoms such as chest pain, shortness of breath, or numbness in the arm.
Your primary care physician can perform an initial evaluation and refer you to a specialist if needed. Orthopedic surgeons and sports medicine physicians have the greatest expertise in diagnosing and managing rotator cuff conditions. Physical therapists with a specialty in musculoskeletal or sports rehabilitation are invaluable partners in both the conservative treatment and the post-surgical recovery process. Do not wait until your rotator cuff problem becomes a crisis — earlier intervention consistently leads to better outcomes.
Conclusion: Taking Control of Your Rotator Cuff Health
The rotator cuff is a remarkable structure, capable of withstanding the extraordinary demands of both everyday life and elite athletic performance. Yet it is also vulnerable, particularly in the context of aging, overuse, and trauma. The good news is that with the right knowledge and care, most rotator cuff problems can be successfully treated, and many can be prevented altogether.
Whether you are managing a mild case of rotator cuff tendinitis or navigating the long road of recovery after a major repair surgery, the principles remain the same: respect the healing process, commit to rehabilitation, work with qualified healthcare professionals, and be patient with your body. The shoulder is a complex joint, and true recovery — particularly after surgery — takes time. But the investment is worthwhile. A healthy, well-functioning rotator cuff is fundamental to so much of what we love to do, from throwing a ball with a child to reaching for a jar on a high shelf.
Armed with the knowledge in this guide, you are now better equipped to recognize rotator cuff problems early, make informed decisions about treatment, and take proactive steps to protect your shoulder health for years to come. If you are in doubt about any shoulder symptoms you are experiencing, do not hesitate to seek professional advice. Your rotator cuff will thank you.
The teres minor is a small but important muscle that works in concert with the infraspinatus. It originates from the lateral border of the scapula and assists with external rotation and adduction of the arm. While the teres minor is less frequently injured than the supraspinatus, its role in overall shoulder stability should not be underestimated.
The subscapularis is the largest and strongest rotator cuff muscle, located on the front (anterior) surface of the scapula. Unlike the other three muscles, it performs internal rotation, pulling the arm toward the body and across the chest. The subscapularis also acts as a critical stabilizer, preventing the humeral head from dislocating anteriorly. Subscapularis tears, while less common, are serious injuries that often require surgical intervention.
Common Rotator Cuff Injuries: Types, Causes, and Risk Factors
Rotator cuff injuries exist on a wide spectrum, from mild tendinitis to complete, full-thickness tears. Understanding the type of injury is essential for determining the most appropriate course of treatment. Healthcare providers classify rotator cuff injuries based on their severity, location, and the mechanism of injury.
Rotator Cuff Tendinitis and Bursitis
Rotator cuff tendinitis refers to inflammation of one or more rotator cuff tendons, typically occurring as a result of overuse or repetitive overhead activities. The condition often develops gradually, beginning with mild discomfort that worsens over time if left untreated. Bursitis — inflammation of the fluid-filled bursa sacs that cushion the tendons — frequently accompanies tendinitis, creating the condition known as shoulder impingement syndrome. In impingement syndrome, the rotator cuff tendons are compressed between the humeral head and the acromion during arm elevation, causing pain, swelling, and progressive tissue damage.
Partial Rotator Cuff Tears
A partial rotator cuff tear is a tear that does not completely sever the tendon. The tendon remains attached to the bone, but its structural integrity is compromised, leading to weakness and pain. Partial tears are further classified based on their location: bursal-side tears affect the upper surface of the tendon (closer to the bursa), articular-side tears affect the lower surface (closer to the joint), and intratendinous tears occur within the substance of the tendon itself. Research suggests that articular-side partial tears are the most common type, likely due to the poorer blood supply to this region and the increased tensile loads it bears during arm motion.
Full-Thickness Rotator Cuff Tears
A full-thickness tear, also called a complete tear, extends through the entire thickness of the tendon, creating a hole or gap that completely disconnects the tendon from the bone. Full-thickness tears range in size from small (less than 1 cm) to massive (greater than 5 cm, often involving multiple tendons). Massive rotator cuff tears represent some of the most challenging shoulder conditions to treat, frequently accompanied by muscle atrophy, fatty infiltration, and superior migration of the humeral head. The incidence of full-thickness rotator cuff tears increases dramatically with age: studies using MRI and ultrasound imaging suggest that approximately 25% of individuals in their 60s and more than 50% of individuals in their 80s have a full-thickness tear, many of which may be asymptomatic.

Causes and Risk Factors for Rotator Cuff Injury
Rotator cuff injuries arise from two primary mechanisms: acute trauma and chronic degeneration. Acute tears often result from a single traumatic event, such as a fall onto an outstretched arm, a forceful pull or lift, or a direct blow to the shoulder. These acute injuries are more common in younger, more physically active individuals. Degenerative tears, on the other hand, develop gradually over years of wear and tear, repetitive overhead activity, and natural age-related changes in tendon blood supply and tissue quality.
Key risk factors for rotator cuff injury include age (especially over 40), occupations involving repetitive overhead work (such as painting, carpentry, or warehouse work), participation in sports that require throwing, swimming, or racquet use, previous shoulder injuries, smoking (which impairs blood supply to tendons), obesity, and a family history of rotator cuff disease. Certain anatomical features, such as a hooked or curved acromion shape (Type II or Type III), narrow subacromial space, or shoulder muscle imbalances, can also predispose individuals to rotator cuff pathology.
Recognizing the Symptoms of a Rotator Cuff Problem
Recognizing rotator cuff symptoms early is crucial for preventing a minor problem from becoming a major one. The symptoms of a rotator cuff injury vary depending on the severity and type of damage, but certain patterns are common across most presentations.
The most common symptom is a dull, aching pain in the outer shoulder and upper arm, which may radiate down toward the elbow. The pain is often worst at night, particularly when lying on the affected shoulder, making sleep difficult. Many patients also report increased pain with specific movements, especially reaching overhead, reaching behind the back, or lifting objects away from the body. A painful arc of motion — pain that occurs between 60 and 120 degrees of arm abduction — is a classic sign of rotator cuff tendinopathy or impingement syndrome.
Arm weakness is another hallmark symptom, particularly difficulty raising or rotating the arm. In cases of acute full-thickness tear, the arm weakness can be so profound that the patient cannot lift the arm at all, a condition known as a "drop arm" sign. Crepitus — a crackling or grinding sensation in the shoulder — may also be present, particularly with rotator cuff tears accompanied by degenerative changes. It is important to note that not all rotator cuff tears are painful; a significant proportion of complete tears, especially in older individuals, are discovered incidentally on imaging performed for other reasons.
How Is a Rotator Cuff Injury Diagnosed?
Diagnosing a rotator cuff injury requires a thorough evaluation that typically combines a careful patient history, a physical examination, and diagnostic imaging. A skilled clinician can often make a presumptive diagnosis based on history and physical exam alone, but imaging studies are typically needed to confirm the diagnosis, assess the severity of the injury, and guide treatment decisions.