Rotator Cuff Muscles: Anatomy, Function, and How to Keep Them Healthy
Introduction to the Rotator Cuff Muscles
The rotator cuff is one of the most talked-about anatomical structures in sports medicine, orthopedics, and physical therapy — and for good reason. This intricate group of four muscles and their associated tendons forms the dynamic cornerstone of shoulder stability, enabling the most mobile joint in the human body to function with both power and precision. Whether you are an elite overhead athlete, a weekend recreational player, an office worker who spends hours at a desk, or simply someone who wants to maintain shoulder health as the years go by, understanding the rotator cuff muscles is fundamental to protecting one of your most essential anatomical assets.
Despite being universally recognized by name, the rotator cuff muscles are often poorly understood — even by people who have been diagnosed with a rotator cuff injury. Many patients know they have "something wrong with their rotator cuff" without having any clear picture of what the rotator cuff actually is, what each of its component muscles does, or why this particular group of muscles is so vulnerable to injury. This lack of understanding can make it harder to engage meaningfully with treatment, to follow through on rehabilitation, or to take preventive action before a minor problem becomes a major one.
This comprehensive guide aims to change that. We will explore the anatomy of each rotator cuff muscle in depth, explain the unique role that each one plays in shoulder movement and stability, examine how these muscles are commonly injured and what those injuries feel like, and outline the most effective exercises and strategies for strengthening and protecting the rotator cuff throughout life.
Overview of the Shoulder Joint
To appreciate the role of the rotator cuff muscles, it helps to first understand the shoulder joint itself. The shoulder — technically a complex of several joints, including the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, and the scapulothoracic articulation — is the most mobile joint in the human body. The glenohumeral joint, which most people refer to when they say "the shoulder joint," is a ball-and-socket joint formed by the head of the humerus (the upper arm bone) and the glenoid fossa of the scapula (the shallow cup-shaped cavity of the shoulder blade).
This ball-and-socket configuration allows the arm to move in virtually all directions — forward, backward, sideways, and in rotation — a range of motion unmatched by any other joint in the body. However, this extraordinary mobility comes with a significant trade-off: stability. Unlike the hip joint, where a deep socket tightly cradles a large femoral head, the glenoid fossa is remarkably shallow — often compared to a golf tee supporting a golf ball. The humeral head contacts only a small portion of the glenoid surface at any given time, making the glenohumeral joint inherently lax and dependent on surrounding soft tissue structures for stability.
This is where the rotator cuff muscles become indispensable. Acting together as a dynamic stabilizing cuff around the humeral head, these four muscles compress the ball firmly into the socket throughout all shoulder movements, preventing the humeral head from sliding or rolling out of position while simultaneously enabling the precise, coordinated motion that the shoulder is capable of. The rotator cuff essentially substitutes dynamic muscular stability for the structural bony stability that other joints like the hip enjoy.
The Four Rotator Cuff Muscles: A Detailed Guide
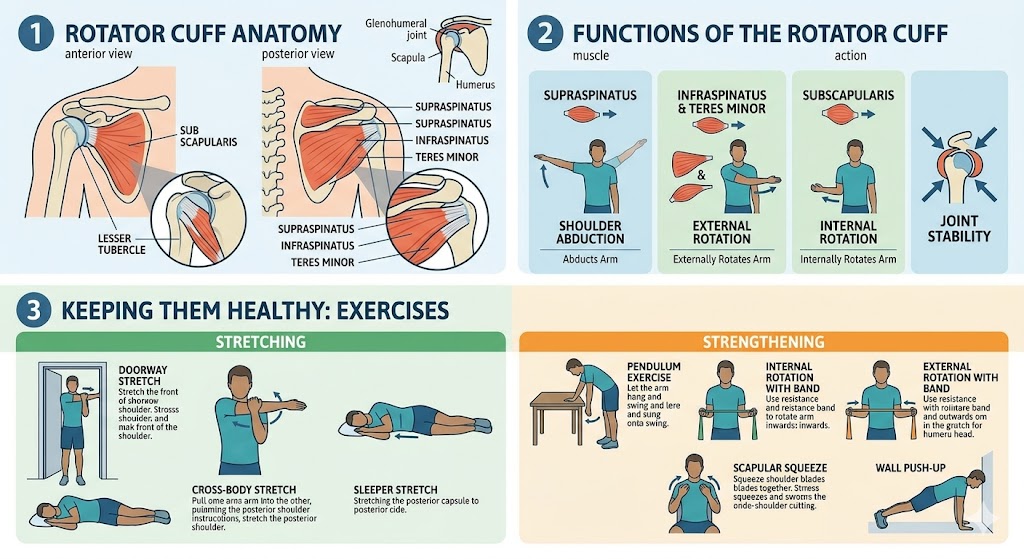
1. Supraspinatus
The supraspinatus is often considered the most clinically significant of the four rotator cuff muscles, partly because it is the most frequently injured and partly because of its critical role in initiating arm elevation. The name "supraspinatus" derives from its location — "supra" meaning above, and "spinatus" referring to the spine of the scapula, the prominent bony ridge that runs diagonally across the back of the shoulder blade. The supraspinatus originates from the supraspinous fossa, the relatively flat area of the scapula above this spine, and its tendon passes beneath the acromion (the bony projection at the top of the shoulder blade) before attaching to the superior facet of the greater tuberosity of the humerus.
The primary function of the supraspinatus is to initiate abduction of the arm — the movement of raising the arm away from the side of the body. Specifically, the supraspinatus is most active during the first 15 to 30 degrees of arm elevation, working in conjunction with the deltoid muscle to lift the arm from its resting position. Without the supraspinatus, initiating this movement is significantly impaired, though the deltoid can take over to complete the arc of elevation once motion has begun. The supraspinatus also plays an essential role in stabilizing the humeral head during arm movement, counteracting the upward pull of the deltoid to prevent superior translation of the humeral head that would otherwise cause impingement of the tendons against the acromion.
The supraspinatus tendon passes through the subacromial space — the narrow corridor between the humeral head below and the coracoacromial arch above — making it uniquely vulnerable to mechanical compression and wear. This anatomical positioning explains why the supraspinatus is the most commonly torn rotator cuff tendon, particularly at the critical zone of the tendon just proximal to its insertion point, where blood supply is reduced and mechanical stress is concentrated. Age-related degeneration of the supraspinatus tendon begins as early as the fourth decade of life and progresses steadily, making supraspinatus tears increasingly common as people age.
2. Infraspinatus
The infraspinatus is the second largest of the rotator cuff muscles and occupies the infraspinous fossa — the large, triangular area of the scapula below the spine. "Infra" means below, reflecting its location beneath the scapular spine. The infraspinatus tendon passes posteriorly and laterally to attach to the middle facet of the greater tuberosity of the humerus, just below the supraspinatus attachment.
The primary action of the infraspinatus is external rotation of the humerus — turning the arm outward so that the thumb points away from the body when the elbow is flexed at 90 degrees. This is one of the most fundamental movements of the shoulder, involved in activities ranging from throwing a baseball and serving a tennis ball to reaching for objects behind the body and positioning the arm during swimming strokes. External rotation strength generated by the infraspinatus is essential for both performance and injury prevention in all overhead athletes.
Beyond its role in producing external rotation, the infraspinatus is critically important as a dynamic stabilizer of the posterior shoulder. During arm elevation and particularly during the deceleration phase of throwing — when the arm must be rapidly slowed down after ball release — the infraspinatus generates powerful eccentric contractions (muscle contractions that occur while the muscle is lengthening) to control humeral head movement and protect the posterior capsule and labrum from excessive stress. The repetitive high-force eccentric loading of the infraspinatus during overhead sport activities is a major contributor to posterior rotator cuff fatigue, tendinopathy, and partial tears in athletes.
Infraspinatus tears, while less common than supraspinatus tears, are frequently identified on MRI studies and often occur in conjunction with supraspinatus pathology. Isolated infraspinatus tears are more commonly seen in overhead athletes and can be challenging to detect clinically, as patients may compensate effectively for moderate infraspinatus weakness by adjusting throwing mechanics or using alternative movement strategies.
3. Teres Minor
The teres minor is the smallest of the four rotator cuff muscles and is sometimes overlooked in discussions of rotator cuff anatomy, yet it plays important and distinct roles in shoulder function. The word "teres" comes from the Latin for "rounded" or "cylindrical," describing the shape of this elongated muscle. The teres minor originates from the lateral border (outer edge) of the scapula and travels upward and laterally to attach to the inferior facet of the greater tuberosity of the humerus — the attachment point just below that of the infraspinatus.
Like the infraspinatus, the teres minor is a powerful external rotator of the humerus. In fact, the teres minor and infraspinatus function so similarly that they are often discussed together as the "external rotators" of the shoulder. The teres minor tends to be most active during external rotation performed with the arm in positions of greater elevation (above shoulder height), making it particularly important during overhead throwing, racket sports, and swimming. In addition to external rotation, the teres minor assists in adduction of the arm (pulling the arm toward the body) and contributes to posterior glenohumeral stabilization, working alongside the infraspinatus to resist anterior translation of the humeral head during forward arm movements.
The teres minor is innervated by the axillary nerve, which distinguishes it from the rest of the rotator cuff muscles (all of which are innervated by branches of the posterior cord of the brachial plexus other than the axillary nerve's contribution). This distinct innervation means that axillary nerve injuries — such as those occurring from shoulder dislocations or direct trauma to the posterolateral shoulder — can specifically affect teres minor function while sparing the other rotator cuff muscles. Isolated teres minor tears are relatively uncommon but have been increasingly recognized in the literature, particularly in overhead athletes, and are associated with a clinical finding known as the "Hornblower's sign" — an inability to maintain external rotation of the arm when it is elevated in the plane of the scapula.
4. Subscapularis
The subscapularis is the largest and strongest of the four rotator cuff muscles and is unique in its location on the anterior (front) surface of the shoulder blade. While the other three rotator cuff muscles are all located on the posterior (back) of the scapula and approach the humerus from behind, the subscapularis lies between the anterior surface of the scapula and the chest wall, passing in front of the shoulder joint to attach to the lesser tuberosity of the humerus — the smaller bony prominence on the front of the humeral head.
The primary action of the subscapularis is internal rotation of the humerus — turning the arm inward so that the thumb points toward the body when the elbow is bent. Internal rotation is involved in a surprising number of daily activities and athletic movements, including tucking in a shirt, reaching behind the back, performing push-ups, throwing motions (the cocking and acceleration phases), swimming freestyle and butterfly strokes, and any activity requiring forceful pushing or pressing movements with the arm.
Beyond its role in producing internal rotation, the subscapularis is the primary anterior stabilizer of the glenohumeral joint. Together with the anterior capsule and the glenohumeral ligaments, the subscapularis tendon forms the primary soft-tissue barrier preventing anterior dislocation of the humeral head during arm movements. This stabilizing role is most critical during positions of shoulder abduction and external rotation — the "cocked" position in throwing — where the anterior structures are placed under maximum tension. A torn or dysfunctional subscapularis significantly compromises anterior shoulder stability and is a major contributor to shoulder instability and recurrent dislocation in some patient populations.
Subscapularis tears have historically been underdiagnosed compared to tears of the other rotator cuff muscles, partly because they occur on the front of the shoulder and are therefore less accessible to physical examination maneuvers than posterior cuff tears, and partly because specific clinical tests for subscapularis integrity (the Belly Press Test, the Bear Hug Test, and the Lift-Off Test) are less well-known than tests for the supraspinatus or infraspinatus. However, with improvements in MRI and ultrasound techniques, subscapularis tears are being identified with increasing frequency, and it is now recognized that they represent a significant proportion of all rotator cuff pathology.
How the Rotator Cuff Muscles Work Together
While it is instructive to consider each rotator cuff muscle individually, in reality these muscles function as an integrated unit, with each contributing to the overall stability and mobility of the shoulder in ways that are deeply interdependent. The concept of the "force couple" is central to understanding how the rotator cuff works as a system. A force couple occurs when two or more forces acting in different directions produce a net rotational effect without translating the joint.
In the shoulder, two key force couples operate to maintain joint stability during arm elevation. In the coronal plane (the plane of arm abduction), the superior rotator cuff (primarily the supraspinatus) and the inferior rotator cuff (infraspinatus and teres minor) work as a force couple to compress the humeral head into the glenoid and counterbalance the upward pull of the deltoid, preventing the humeral head from riding up and impinging on the acromion. In the transverse plane (the horizontal plane of rotation), the anterior rotator cuff (subscapularis) and the posterior rotator cuff (infraspinatus and teres minor) form a force couple that balances the rotational forces acting on the shoulder during dynamic arm movements.
This coordinated action requires not only sufficient strength in each individual muscle but also precise neuromuscular timing — the ability of the nervous system to activate each muscle at exactly the right moment and to the right degree during dynamic shoulder movements. Research has shown that rotator cuff muscle activation begins before the arm even starts to move (a phenomenon known as "pre-activation" or "feedforward control"), demonstrating that these muscles are not simply reacting to movement but are proactively preparing the joint for the loads it is about to experience. Disruption of this neuromuscular coordination — whether due to injury, fatigue, pain, or disuse — is a major contributor to shoulder dysfunction and ongoing rotator cuff pathology.
Common Causes of Rotator Cuff Muscle Injury
The rotator cuff muscles are vulnerable to injury through several distinct mechanisms, and understanding these can help both in prevention and in making sense of how an injury developed. Acute traumatic injuries typically involve a sudden, forceful overload of one or more rotator cuff tendons — such as catching a heavy falling object, breaking a fall with an outstretched arm, or experiencing a sudden jerk or pull on the arm. These acute injuries are most common in younger, more active individuals and tend to involve the supraspinatus, though any tendon can be affected depending on the direction of the force.
Repetitive microtrauma, or overuse injury, is a more insidious but equally common mechanism of rotator cuff damage. Activities that require repeated overhead arm movements — pitching, swimming, tennis, painting, carpentry, assembly line work — place cyclical loading on the rotator cuff tendons that, over time, exceeds the tendons' capacity to repair themselves. The result is progressive tendon degeneration, micro-tearing, and eventually partial or complete tears. The supraspinatus is most commonly affected by this mechanism, though the infraspinatus and subscapularis are also frequently involved in overhead athletes.
Degenerative aging changes are the most prevalent cause of rotator cuff tears in the general population. Beginning in the fourth decade of life, the rotator cuff tendons undergo progressive histological changes — loss of organized collagen architecture, decreased cellularity, accumulation of calcific deposits, and reduced vascularity in the critical zone of the supraspinatus tendon. These degenerative changes reduce the mechanical strength and elasticity of the tendons, making them increasingly susceptible to tearing even with relatively minor stresses. By the sixth and seventh decades of life, full-thickness rotator cuff tears are present in a substantial proportion of the population, many of whom experience no symptoms.
Shoulder impingement — the mechanical compression of the rotator cuff tendons between the humeral head and the coracoacromial arch — is a major contributing factor to rotator cuff pathology in all age groups. Factors that contribute to impingement include acromial morphology (certain shapes of the acromion, particularly a hooked or curved acromion, narrow the subacromial space), acromioclavicular joint arthritis with inferior osteophyte formation, poor scapular mechanics due to weakness of the scapular stabilizing muscles, and postural abnormalities such as rounded shoulders and forward head posture.
Exercises to Strengthen the Rotator Cuff Muscles
Strengthening the rotator cuff muscles is one of the most important things anyone can do for long-term shoulder health, whether as injury prevention, as part of a rehabilitation program, or as performance enhancement for athletes. The following exercises target the individual rotator cuff muscles and the shoulder as a functional unit. All should be performed with controlled, deliberate technique, starting with light resistance and progressing gradually.
External Rotation with Resistance Band
This exercise is one of the most fundamental and widely recommended rotator cuff strengthening movements, targeting primarily the infraspinatus and teres minor. Stand with the elbow of the exercising arm bent to 90 degrees and held close to the side of the body, holding a resistance band anchored to a fixed point at elbow height. Keeping the elbow pinned against the side, slowly rotate the forearm outward away from the body against the resistance of the band, then return to the starting position under control. Perform 3 sets of 15-20 repetitions on each side. The key to this exercise is maintaining the elbow position and performing the movement slowly — rushing through the motion reduces the effectiveness and increases injury risk.
Internal Rotation with Resistance Band
The counterpart to external rotation, this exercise targets the subscapularis muscle. Position the resistance band at elbow height on the opposite side of the exercising arm. With the elbow bent at 90 degrees and held close to the side, slowly rotate the forearm inward toward the abdomen against the band's resistance, then return to the starting position under control. This exercise is particularly important for restoring balanced strength in patients with anterior shoulder instability or subscapularis pathology.
Side-Lying External Rotation
This gravity-resisted exercise isolates the infraspinatus and teres minor effectively without requiring any equipment. Lie on the side with the top arm bent to 90 degrees at the elbow, elbow resting against the side of the body, and a light dumbbell in the hand. Keeping the elbow pinned against the body, slowly rotate the forearm upward toward the ceiling, pause briefly at the top, then lower under control. This is an excellent exercise for individuals recovering from posterior rotator cuff injuries or for those who find resistance band setups inconvenient.
Prone Y, T, and W Exercises
These exercises, performed lying face down on a flat surface or an exercise bench with the arms hanging freely, target the rotator cuff muscles in combination with the important scapular stabilizing muscles (lower trapezius, middle trapezius, and rhomboids). For the Y, raise both arms diagonally overhead in the shape of a Y, thumbs pointing up. For the T, raise both arms straight out to the sides at shoulder height in a T shape. For the W, draw the arms back into a W shape by bending the elbows and squeezing the shoulder blades together. All three movements should be performed slowly with light resistance (or bodyweight alone initially) and held briefly at the top position before lowering.
Empty Can Exercise (Supraspinatus Isolation)
The empty can exercise specifically targets the supraspinatus muscle, making it invaluable for both rehabilitation and prevention. Stand with the arm extended, thumb pointing downward (as if emptying a can), and the arm positioned at approximately 30 to 45 degrees in front of the body (in the "scapular plane"). Elevate the arm to shoulder height against resistance — a light dumbbell or resistance band — then lower under control. This movement pattern reduces acromial impingement compared to straight-plane abduction and provides excellent isolated loading of the supraspinatus tendon.
Sleeper Stretch
While not a strengthening exercise per se, the sleeper stretch is one of the most important flexibility exercises for rotator cuff health, specifically targeting the posterior shoulder capsule and infraspinatus/teres minor flexibility. Tight posterior shoulder structures are a major contributor to impingement and altered glenohumeral mechanics in overhead athletes. Lie on the side on the affected shoulder, with the shoulder at 90 degrees of flexion and the elbow bent to 90 degrees. Using the opposite hand, gently push the forearm downward toward the floor (into internal rotation), maintaining a comfortable stretch in the posterior shoulder. Hold for 30 seconds and repeat three times on each side.
Scapular Stabilization Exercises
No rotator cuff strengthening program is complete without attention to the scapular stabilizing muscles. The rotator cuff can only function effectively when the scapula — which serves as its moving platform — is properly positioned and controlled. Weakness in the lower and middle trapezius, serratus anterior, and rhomboids leads to poor scapular mechanics that increase subacromial impingement and alter the biomechanics of every rotator cuff exercise. Wall slides, scapular push-ups, and prone row variations are all excellent exercises for building the scapular stability that underlies effective rotator cuff function.
The Role of the Rotator Cuff in Athletic Performance
For athletes — particularly those involved in overhead sports — the rotator cuff muscles are among the most performance-critical structures in the body. In baseball pitching, for example, the external rotators (infraspinatus and teres minor) must eccentrically decelerate the arm during follow-through with forces estimated to approach 100% of body weight — making the posterior rotator cuff one of the most heavily loaded muscular structures in any sport. In swimming, each stroke cycle places the rotator cuff tendons under repetitive compressive and tensile loading, with elite swimmers performing hundreds of thousands of stroke cycles per year. In tennis, the serve requires rapid concentric contraction of the subscapularis during the acceleration phase, followed by powerful eccentric loading of the posterior cuff during deceleration.
Optimizing rotator cuff muscle function for athletic performance requires a nuanced approach that goes beyond simple strengthening. Eccentric training — in which the muscles are specifically trained to generate force while lengthening — is particularly important for overhead athletes, as it directly targets the most demanding aspect of rotator cuff loading that occurs during the deceleration phase of throwing and serving. Neuromuscular training that emphasizes the timing and coordination of rotator cuff activation, rather than simply building maximal strength, is equally critical. And periodization — the systematic variation of training load, intensity, and volume over time — helps prevent the cumulative overloading that leads to rotator cuff overuse injuries in athletes at all levels.
Rotator Cuff Muscle Health Across the Lifespan
The health and function of the rotator cuff muscles change considerably across the lifespan, and an understanding of these changes can inform age-appropriate prevention and management strategies. In children and adolescents, the rotator cuff tendons are generally robust and resilient, but the growth plates of the shoulder (particularly the proximal humeral physis) can be vulnerable to overuse stress, particularly in young overhead athletes who throw at high volumes. "Little leaguer's shoulder" — a stress injury to the proximal humeral growth plate — is an important consideration in youth baseball players who present with shoulder pain.
In young and middle-aged adults, rotator cuff injuries are most commonly related to overuse, acute trauma, or some combination of both. Maintaining adequate rotator cuff strength and flexibility, using proper throwing and lifting mechanics, and managing training loads carefully are the most effective preventive strategies in this age group. In older adults, the focus shifts increasingly toward managing the degenerative changes that are occurring regardless of activity level, maintaining adequate strength and range of motion to preserve function, and identifying and treating symptomatic tears before they progress to massive, irreparable damage. Even in the presence of confirmed rotator cuff tears, regular exercise and physical therapy can significantly improve function, reduce pain, and delay or avoid the need for surgical intervention in many older patients.
When to Seek Professional Help
Understanding the rotator cuff muscles and their vulnerabilities empowers you to take a proactive role in your shoulder health, but it is equally important to know when professional evaluation is needed. Shoulder pain that persists for more than two to three weeks despite rest and over-the-counter pain medication, weakness in shoulder elevation or rotation that is interfering with daily activities, pain that regularly disrupts sleep, or any sudden onset of significant shoulder pain and weakness following a traumatic event should all prompt evaluation by a healthcare provider.
An orthopedic surgeon, sports medicine physician, or physical therapist with expertise in shoulder conditions can perform a thorough evaluation to determine the cause of your symptoms and develop an appropriate treatment plan. Early intervention — before a minor tendinopathy progresses to a significant tear, or before muscle atrophy and stiffness complicate the clinical picture — consistently produces better outcomes than delayed treatment. Do not dismiss shoulder pain as an inevitable consequence of aging or activity; in many cases, targeted treatment and rehabilitation can restore full function and significantly improve quality of life.
Conclusion
The rotator cuff muscles — supraspinatus, infraspinatus, teres minor, and subscapularis — are four remarkable structures that, working in concert, make the extraordinary mobility and power of the human shoulder possible. Each muscle has its own unique anatomy, its own primary actions, and its own specific vulnerabilities, yet together they form an integrated system of dynamic stabilization that is far greater than the sum of its parts. Understanding how these muscles work, why they are prone to injury, and what can be done to strengthen and protect them is not just academically interesting — it is genuinely actionable knowledge that can make a meaningful difference in your shoulder health, your athletic performance, and your quality of life.
Whether you are recovering from a rotator cuff injury, trying to prevent one, or simply curious about the anatomy that allows you to reach, lift, throw, and perform the countless daily activities that healthy shoulders make possible, the knowledge you have gained from this guide provides a solid foundation. Take care of your rotator cuff muscles — they are working hard every single day to keep your shoulder stable, strong, and moving freely.