Rotator Cuff Pain: Causes, Relief Strategies, and When to See a Doctor
What Is Rotator Cuff Pain?
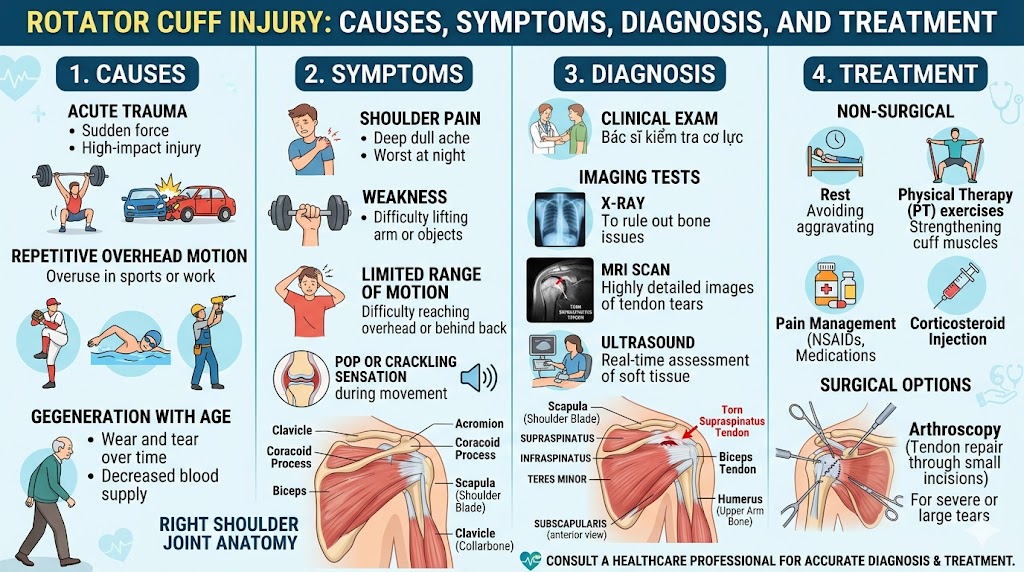
Rotator cuff pain is one of the most common musculoskeletal complaints in the world, affecting millions of people each year across all age groups, activity levels, and occupations. It is a broad term that encompasses any pain originating from or closely related to the four-muscle group — the supraspinatus, infraspinatus, teres minor, and subscapularis — that surrounds the glenohumeral (shoulder) joint and is responsible for both stabilizing and moving the arm. Whether it manifests as a dull, persistent ache after a long day at the office, a sharp pain when reaching overhead in the kitchen, or a searing discomfort that prevents sleep, rotator cuff pain can range from mildly inconvenient to severely debilitating.
What makes rotator cuff pain particularly challenging — both to experience and to manage — is its remarkable variability. Two individuals with identical rotator cuff damage can experience completely different levels of pain, functional limitation, and impact on daily life. Conversely, someone with severe, life-disrupting shoulder pain may be found to have only minor tendon changes on imaging, while another person with a massive complete tear of the rotator cuff may report relatively little pain. This disconnect between structural damage and pain experience reflects the complex, multidimensional nature of pain itself — and it underscores the importance of treating the person rather than simply the imaging findings.
This comprehensive guide will take you through everything you need to know about rotator cuff pain: what causes it, where it tends to be felt, how it changes over time, what makes it worse, and — most importantly — what can be done to relieve it, rehabilitate it, and prevent it from returning. Whether you are in the early stages of a shoulder problem or have been struggling with chronic rotator cuff pain for years, the information and strategies contained here can help you take meaningful, informed action toward recovery.
The Nature of Rotator Cuff Pain: Where It Hurts and Why
Understanding the character and location of rotator cuff pain is one of the most important tools for identifying it correctly and distinguishing it from other sources of shoulder discomfort. Rotator cuff pain has several distinctive features that, when recognized together, strongly suggest a rotator cuff origin.
In terms of location, rotator cuff pain is most classically felt on the lateral (outer) aspect of the upper arm, roughly over the deltoid muscle, and at the front and top of the shoulder. Many patients point to the side of their shoulder rather than the joint itself when asked to indicate where the pain is. The pain frequently radiates down the outer arm, sometimes reaching as far as the elbow, and occasionally patients report discomfort that extends into the forearm or hand — though this distal radiation is less typical of pure rotator cuff pain and may suggest concurrent nerve involvement.
Posterior (back of shoulder) pain can also be a feature of rotator cuff pathology, particularly when the infraspinatus or teres minor tendons are involved, or when secondary posterior capsule tightness has developed. Some patients experience pain that wraps around the shoulder in a diffuse pattern that is difficult to localize precisely, while others report very specific, point-tender areas that they can identify exactly. Pain that primarily involves the neck, the trapezius muscle, or radiates in a clearly dermatomal pattern down the arm and into the fingers is more likely to originate from the cervical spine and should be evaluated accordingly.
The quality of rotator cuff pain varies with the underlying pathology. Tendinitis and mild partial tears typically produce a dull, aching, nagging quality of pain that is worse with activity and better at rest — at least initially. More significant partial tears and complete tears can produce sharper, more intense pain, particularly during specific provocative movements. Acute traumatic tears present with sudden, severe pain that patients often describe as an immediate burning or tearing sensation at the moment of injury. Chronic degenerative tears may produce a more constant, boring ache that fluctuates with activity level but never fully resolves.
Common Causes of Rotator Cuff Pain
Rotator Cuff Tendinitis and Impingement
Rotator cuff tendinitis — inflammation of one or more of the rotator cuff tendons — is among the most frequent causes of shoulder pain in adults and is often the earliest stage in a continuum of rotator cuff pathology. It is closely linked to the concept of shoulder impingement syndrome, in which the rotator cuff tendons are mechanically compressed or pinched in the narrow subacromial space between the humeral head below and the acromion (the bony roof of the shoulder) above.
Impingement and the resulting tendinitis are typically provoked or worsened by repetitive overhead activities — anything that requires raising the arm above shoulder height repeatedly or sustaining overhead positions for extended periods. Occupations at highest risk include painters, carpenters, electricians, hairdressers, assembly workers, and anyone whose job requires sustained or repeated arm elevation. Overhead athletes — baseball pitchers, volleyball players, swimmers, tennis players, and gymnasts — are also at significantly elevated risk. Even desk workers who maintain prolonged postures with rounded shoulders and forward head position can develop impingement-related tendinitis through the subtle but cumulative mechanical effects of poor alignment on subacromial space dimensions.
The pain of rotator cuff tendinitis typically builds gradually over days to weeks or months, and is initially felt only during or immediately after provocative activities. As the condition progresses, the pain may begin to intrude on rest periods and eventually on sleep, signaling a transition from mild, activity-related tendinitis to a more established and potentially more structurally significant problem.
Rotator Cuff Tears
Tears of the rotator cuff tendons are a major source of rotator cuff pain and represent a more advanced form of rotator cuff pathology. Tears can be classified by thickness (partial vs. full-thickness), by which tendon is involved, by size, and by their cause (traumatic vs. degenerative). Each of these characteristics influences the pain experience in ways that are clinically meaningful.
Partial thickness tears, in which only a portion of the tendon's cross-sectional area is disrupted, can range from tiny, almost subclinical defects to large, nearly complete tears that are only millimeters away from full-thickness status. The pain associated with partial tears is often indistinguishable from tendinitis, though it tends to be more persistent and more resistant to initial conservative measures. Specific movements that place tension directly on the involved tendon — such as resisted external rotation for infraspinatus tears, or resisted abduction in the plane of the scapula for supraspinatus tears — may elicit particularly sharp, well-localized pain that can help clinicians identify the affected structure.
Full-thickness tears, where the tendon is completely divided, may paradoxically be associated with less pain than one might expect, particularly in the setting of longstanding degenerative tears. This is because the nervous tissue in severely degenerated tendons may be partially compromised, and because the surrounding structures adapt over time to the altered shoulder mechanics. However, large complete tears are commonly associated with significant pain, particularly at night, as well as dramatic functional deficits that are often the primary driver for seeking treatment.
Acute traumatic tears — which may be complete from the outset, particularly in younger individuals — typically cause immediate, severe pain that is qualitatively different from the insidious discomfort of degenerative pathology. Patients often describe feeling or hearing a "pop" at the moment of the injury, followed by sharp, burning pain and rapid loss of shoulder function. This acute presentation is a medical urgency that warrants prompt evaluation.
Subacromial Bursitis
The subacromial bursa is a fluid-filled sac that sits between the rotator cuff tendons and the undersurface of the acromion, providing cushioning and reducing friction as the tendons glide during arm movement. When this bursa becomes inflamed — a condition known as subacromial bursitis — it can be an independent and highly significant contributor to rotator cuff pain. Bursitis rarely occurs in isolation; it most commonly develops as a secondary response to underlying rotator cuff tendinitis or tearing, as the inflammatory mediators produced by a damaged tendon spread to the adjacent bursal tissue.
Subacromial bursitis produces a characteristic pattern of pain that is particularly intense at the anterior and lateral shoulder, exquisitely tender to palpation just beneath the acromion, and dramatically worsened by any attempt to raise the arm — particularly in the mid-range of elevation (roughly 60 to 120 degrees), where the bursa is maximally compressed. In severe cases, even the weight of a hanging arm can produce significant discomfort, and many patients hold the arm close to the body and slightly internally rotated in an instinctive effort to decompress the inflamed structures.
Calcific Tendinitis
Calcific tendinitis is a specific and often dramatically painful form of rotator cuff pathology characterized by the deposition of calcium hydroxyapatite crystals within the substance of the rotator cuff tendons — most commonly the supraspinatus. The exact cause of calcific tendinitis remains incompletely understood, but it appears to involve a process of cell-mediated calcium deposition within areas of tendon tissue that are undergoing a form of fibrocartilaginous transformation, possibly in response to relative hypoxia (reduced oxygen supply).
What makes calcific tendinitis clinically remarkable is the sheer intensity of pain it can produce, particularly during the "resorptive phase" — the period during which the body begins to break down and reabsorb the calcium deposits. During this phase, which may last days to weeks, the shoulder pain can be absolutely excruciating, requiring strong analgesics and sometimes emergency intervention. Between episodes, patients may experience relatively mild, activity-related pain that is easy to dismiss, only to be blindsided by a sudden, extreme pain exacerbation that brings them to an emergency room convinced they have sustained a major injury.
Biceps Tendon Pathology
The long head of the biceps tendon — which passes through the shoulder joint before attaching to the superior rim of the glenoid labrum — is closely associated with the rotator cuff and frequently contributes to or is confused with rotator cuff pain. Biceps tendinitis, partial tears of the biceps tendon, and superior labral tears (SLAP lesions) all produce anterior shoulder pain in a location that overlaps significantly with the distribution of supraspinatus and subscapularis pain. In many cases, rotator cuff pathology and biceps tendon pathology coexist, since the forces that damage the rotator cuff often similarly stress the biceps tendon. Anterior shoulder pain that is well-localized to the bicipital groove (the groove on the front of the upper humerus through which the biceps tendon passes) and is reproduced by resisted forearm supination or elbow flexion is particularly suggestive of biceps tendon involvement.
Factors That Worsen Rotator Cuff Pain
Identifying the specific activities, positions, and circumstances that exacerbate rotator cuff pain is essential for both accurate diagnosis and effective self-management. While individual presentations vary, several factors consistently emerge as the most common triggers and amplifiers of rotator cuff pain.
Overhead activities are the quintessential provocateur of rotator cuff pain. Any movement that requires raising the arm above shoulder height — reaching for objects on high shelves, washing hair, painting a ceiling, serving in tennis, or swimming freestyle — places the rotator cuff tendons in a position of maximum compression within the subacromial space. The repeated or sustained nature of these movements, rather than any single instance, is typically what transforms a manageable ache into significant pain.
Sleeping positions are a particularly important and often underappreciated factor in rotator cuff pain. Lying on the affected shoulder compresses the inflamed tendons and bursa, dramatically increasing local tissue pressure and pain. Even lying on the opposite side can be problematic, as the affected arm may roll into a position of internal rotation and horizontal adduction that tensions the posterior capsule and external rotators. Many patients find that their worst rotator cuff pain occurs not during the day's activities but in the middle of the night, waking them from sleep and making it impossible to find a comfortable position.
Carrying or lifting objects — particularly when done with the arm extended away from the body, or when involving heavy weights — places significant load through the rotator cuff tendons. Grocery bags, briefcases, tool bags, and even the weight of an arm hanging unsupported can provoke or sustain rotator cuff pain in more acute presentations. Pushing and pulling movements, particularly at or above shoulder height, are similarly provocative.
Certain work-related postures and ergonomic factors consistently contribute to rotator cuff pain in occupational settings. Sustained arm elevation, working with the arms raised above the head, reaching across the body repeatedly, and using vibrating tools all increase the mechanical load on the rotator cuff tendons. Poor workstation setup — such as a keyboard placed too high, a computer monitor at an angle that requires sustained neck or shoulder rotation, or a chair at the wrong height — can create chronic postural stresses that slowly erode rotator cuff tendon health over months and years.
Psychological and psychosocial factors are increasingly recognized as important modulators of rotator cuff pain experience. Stress, anxiety, depression, and catastrophizing (the tendency to interpret pain as more threatening and uncontrollable than it actually is) have all been shown to amplify the experience of musculoskeletal pain, including rotator cuff pain. Poor sleep quality — which is itself often disrupted by rotator cuff pain — can lower the pain threshold through a self-reinforcing cycle that is important to recognize and address as part of comprehensive management.
How Rotator Cuff Pain Changes Over Time
Rotator cuff pain rarely remains static — it tends to evolve over time in ways that reflect both the natural history of the underlying pathology and the individual's response to that pathology. Understanding this trajectory helps set realistic expectations and underscores the importance of timely intervention.
In its early stages, rotator cuff pain is typically activity-related — present during and immediately after provocative movements, but absent at rest. Many people in this stage manage their symptoms through activity modification alone, avoiding the movements that hurt and getting on with their lives. While this approach is understandable, it is often counterproductive in the long run, as it does nothing to address the underlying tendon pathology and may allow it to progress silently.
As rotator cuff pathology advances — whether through continued repetitive stress, age-related degeneration, or an acute injury superimposed on pre-existing damage — the pain begins to intrude on rest and eventually on sleep. This transition from activity-related to rest pain and nocturnal pain typically signals a worsening of the underlying pathology and is often the threshold at which people finally seek medical attention. At this stage, the pain is also more likely to be associated with meaningful functional limitations — difficulty reaching, reduced strength, and compensatory movement patterns that can begin to stress other structures in the shoulder and upper extremity.
In longstanding, untreated rotator cuff pathology, the pain may paradoxically begin to improve as the underlying nerve supply to the severely degenerated tendons diminishes and the surrounding structures adapt to the altered shoulder mechanics. However, this apparent "improvement" in pain masks ongoing structural deterioration and progressive muscle atrophy that significantly compromises the shoulder's long-term function and repairability. This is why pain is an unreliable guide to the severity of rotator cuff pathology, and why professional evaluation — including appropriate imaging — is important for anyone with persistent shoulder pain.
Rotator Cuff Pain Relief: Home Strategies
For most cases of rotator cuff pain — particularly those of mild to moderate severity without complete tears or other structural complications — a combination of intelligent self-management strategies can provide meaningful relief and set the stage for more definitive rehabilitation. The following approaches are well-supported by evidence and are appropriate as initial management while awaiting professional evaluation or as adjuncts to formal treatment.
Activity Modification
The first and most immediate step in managing acute rotator cuff pain is to reduce or eliminate the specific activities that are provoking or worsening it. This does not mean complete rest — total immobilization of the shoulder is generally counterproductive and can lead to secondary stiffness — but rather a thoughtful modification of daily and occupational activities to reduce the mechanical load on the inflamed or damaged tendons. Temporary avoidance of overhead reaching, heavy lifting, repetitive throwing or serving, and sustained arm elevation allows the inflammatory response to settle and prevents the perpetuation of a pain-inflammation cycle that can become self-sustaining.
Ice and Heat Application
Cryotherapy (ice application) is most beneficial in the acute phase of rotator cuff pain — within the first 48 to 72 hours after an injury or during a significant flare-up of chronic symptoms. Applying an ice pack wrapped in a cloth to the shoulder for 15 to 20 minutes, three to four times per day, helps to reduce local inflammation, decrease nerve conduction velocity (which reduces pain signal transmission), and limit secondary tissue swelling. Heat therapy becomes more appropriate once the acute inflammatory phase has subsided, typically after the first few days. The application of moist heat to the shoulder before stretching or exercise improves tissue extensibility and can significantly reduce the pain and stiffness associated with chronic rotator cuff conditions.
Over-the-Counter Pain Relief
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Advil, Motrin) and naproxen sodium (Aleve) are among the most effective over-the-counter options for rotator cuff pain. By inhibiting the production of prostaglandins — key mediators of the inflammatory and pain response — NSAIDs address both the pain and the underlying inflammation simultaneously. For best effect, NSAIDs should be taken regularly (not just as needed) for a defined period — typically one to two weeks — rather than sporadically in response to individual pain episodes. However, they should be used for the shortest duration necessary and with awareness of their potential side effects, particularly gastrointestinal irritation, cardiovascular effects, and renal impairment in susceptible individuals.
Topical NSAIDs (such as diclofenac gel) offer an alternative for individuals who cannot tolerate oral NSAIDs, providing local anti-inflammatory effects with minimal systemic absorption. Topical analgesics containing menthol, capsaicin, or lidocaine may provide temporary symptomatic relief and can be useful as a complement to other management strategies.
Optimizing Sleep Position
Given the notorious impact of rotator cuff pain on sleep quality, developing strategies for more comfortable sleeping is a practical and high-impact component of home management. Sleeping on the unaffected side with a pillow placed between the arms to support the affected shoulder in a neutral position can significantly reduce nocturnal pain. Sleeping on the back with the arm supported on a pillow placed beside the body to maintain slight external rotation is another option that reduces compression and tension on the rotator cuff structures. Avoiding sleeping on the affected shoulder and minimizing positions that allow the arm to roll across the body (into horizontal adduction and internal rotation) are the most consistently helpful adjustments.
Posture Correction and Ergonomics
For individuals whose rotator cuff pain is related to or perpetuated by postural factors — particularly the rounded shoulder, forward head posture common in desk workers and smartphone users — addressing these postural habits can provide significant and lasting relief. Simple postural cues such as gently drawing the shoulder blades together and downward, keeping the chin tucked rather than protruded, and ensuring that the thoracic spine is extended rather than flexed can immediately reduce subacromial pressure and tension on the rotator cuff tendons. Ergonomic adjustments to the workstation — raising or lowering the desk height, repositioning the monitor, adjusting chair height to allow neutral shoulder positioning — address the environmental contributors to poor posture.
Gentle Range of Motion Exercises
Maintaining shoulder mobility through gentle, pain-free range of motion exercises is important even during the acute phase of rotator cuff pain. Pendulum exercises — leaning forward, allowing the affected arm to hang freely, and using gentle body movement to create small circular or pendulum-like motions of the arm — are a well-established, low-load method of maintaining shoulder mobility without stressing the damaged tendons. These exercises are performed with gravity doing the work rather than active muscle contraction, making them safe and accessible even for individuals with significant pain or early post-surgical presentations.
Medical and Therapeutic Treatments for Rotator Cuff Pain
Physical Therapy
Physical therapy is the cornerstone of non-surgical rotator cuff pain management and has a robust evidence base supporting its effectiveness for tendinitis, partial tears, and even some complete tears — particularly in older or less active individuals. A comprehensive physical therapy program for rotator cuff pain addresses multiple interrelated components: reducing pain and inflammation through therapeutic modalities such as ultrasound, electrical stimulation, and manual therapy; restoring full, pain-free range of motion through progressive stretching and joint mobilization; rebuilding rotator cuff and scapular stabilizer strength through a carefully progressed strengthening program; and addressing biomechanical and postural factors that may have contributed to or perpetuated the problem.
The rotator cuff strengthening component of physical therapy is particularly important and should be central to any rehabilitation program. Research consistently shows that a structured, progressive exercise program targeting the rotator cuff muscles and their synergists can produce pain reduction and functional improvement comparable to surgical intervention for many types of rotator cuff pathology. The key is progression — starting with low-load exercises that do not provoke symptoms, and gradually increasing resistance and complexity as the tendon and muscle tissue adapts and heals.
Corticosteroid Injections
When rotator cuff pain is severe enough to prevent meaningful participation in physical therapy, or when the inflammatory component is particularly prominent (as in subacromial bursitis or calcific tendinitis), a corticosteroid injection into the subacromial space can be a valuable adjunct to physical therapy. Delivered by a physician under ultrasound or fluoroscopic guidance, these injections can provide rapid, significant reduction in inflammation and pain — often within days — allowing the patient to engage more fully in rehabilitation exercises that address the underlying mechanical causes of their problem.
It is important to understand that corticosteroid injections address the inflammatory component of rotator cuff pain but do not repair damaged tendon tissue. Their benefit is typically temporary, and the evidence suggests that repeated injections over time may actually weaken tendon tissue and increase the risk of tendon tearing. Most guidelines recommend limiting subacromial corticosteroid injections to a maximum of two to three per shoulder per year, with a minimum of three months between injections, and with the understanding that they are a bridge to rehabilitation rather than a standalone treatment.
Platelet-Rich Plasma (PRP) Injections
Platelet-rich plasma therapy, in which a concentrated preparation of the patient's own blood platelets — rich in growth factors that stimulate tissue healing — is injected into the site of tendon damage, has attracted considerable interest as a potential treatment for rotator cuff pain. The theoretical rationale is compelling: by delivering a concentrated bolus of natural healing factors directly to poorly vascularized tendon tissue, PRP may be able to stimulate the repair processes that the tendon's own inadequate blood supply cannot sustain. Clinical evidence for PRP in rotator cuff pathology is still evolving, with some studies showing meaningful benefits for tendinopathy and partial tears, while others show more modest effects. PRP is generally considered a promising adjunct treatment rather than a first-line or stand-alone therapy.
Surgical Treatment
When conservative measures fail to adequately control rotator cuff pain and restore function after a reasonable trial of several months, or when the nature of the rotator cuff damage is such that surgical repair offers the best prospect for full recovery, surgical intervention becomes appropriate. Arthroscopic rotator cuff repair — the most commonly performed rotator cuff surgery — involves using small instruments and a camera inserted through tiny incisions to reattach the torn tendon to the bone using suture anchors. The procedure is performed under general or regional anesthesia as an outpatient procedure in most cases, and the subsequent rehabilitation program — which may take six months to a year for full recovery — is as important as the surgery itself in determining the final outcome.
Pain relief is one of the most consistent and satisfying outcomes of successful rotator cuff surgery, with the large majority of patients reporting significant or complete resolution of their preoperative pain following repair and rehabilitation. However, it is important to set realistic expectations: surgical repair does not guarantee freedom from all shoulder symptoms, and the outcome depends heavily on the size and chronicity of the tear, the quality of the tendon tissue, the patient's age and overall health, and their commitment to the postoperative rehabilitation program.
Pain Management Strategies for Chronic Rotator Cuff Pain
For individuals living with chronic rotator cuff pain — whether because they are not surgical candidates, have chosen to manage conservatively, or are experiencing pain that persists despite previous treatment — developing effective long-term pain management strategies is essential for maintaining quality of life and functional capacity.
Consistent exercise remains one of the most powerful tools available for managing chronic rotator cuff pain. Regular strengthening of the rotator cuff and periscapular muscles helps to maintain joint stability, reduce impingement, and preserve functional capacity. Aerobic exercise more broadly provides systemic benefits for pain management through the release of endorphins, reduction of systemic inflammation, improvement of sleep quality, and positive effects on mood and psychological wellbeing. Even low-impact activities such as walking, cycling, or water-based exercise can provide meaningful pain management benefits in individuals with chronic shoulder pain.
Mindfulness-based approaches and pain education have an established evidence base for chronic musculoskeletal pain management. Understanding that chronic pain does not always reflect ongoing tissue damage — and that the nervous system's sensitivity can be modulated through cognitive and behavioral strategies — can be genuinely liberating for individuals caught in a cycle of pain-fear-avoidance. Working with a psychologist or pain specialist trained in cognitive behavioral therapy (CBT) or acceptance and commitment therapy (ACT) for chronic pain can complement physical treatments and significantly improve overall quality of life.
Pacing — the deliberate planning and distribution of activities throughout the day to avoid both under-activity and over-activity — is a key principle in chronic pain management that is often underutilized. Learning to identify personal activity thresholds, building in regular rest periods before fatigue and pain escalate, and gradually expanding activity tolerance through structured graded exposure are all components of effective pacing that can break the cycle of boom-and-bust activity patterns that perpetuate chronic rotator cuff pain.
Preventing Rotator Cuff Pain Recurrence
Once rotator cuff pain has been effectively managed, the focus shifts to preventing recurrence — a goal that requires attention to the same factors that originally contributed to the problem. Maintaining a consistent rotator cuff and shoulder strengthening program is the single most important prevention strategy, ensuring that the muscles and tendons remain strong, balanced, and resilient enough to handle the demands of daily life and recreational or occupational activities.
Attention to movement mechanics and ergonomics remains important on an ongoing basis. Continuing to apply the postural and ergonomic principles learned during rehabilitation, and periodically reassessing work and training setups as circumstances change, helps prevent the reemergence of mechanical stressors that originally drove the problem. For overhead athletes and manual workers, periodic check-ins with a physical therapist or sports medicine professional — even in the absence of symptoms — can identify emerging biomechanical issues before they produce pain and can fine-tune conditioning programs to match evolving demands.
Respecting recovery and avoiding training errors that involve sudden, large increases in activity volume or intensity is equally critical. Many rotator cuff pain recurrences occur when individuals who have recovered well become overconfident and return too rapidly to high-demand activities without adequate preparation. Following the principle of gradual, progressive loading — increasing demands by no more than 10 to 15 percent per week — provides the tendons and muscles with the time they need to adapt and remain healthy.
When to See a Doctor for Rotator Cuff Pain
While mild, activity-related rotator cuff pain may resolve with conservative self-management, several situations clearly warrant prompt professional evaluation. You should seek medical attention without delay if you experience sudden severe shoulder pain following a traumatic event — a fall, a direct blow, or a forceful arm movement — particularly if accompanied by immediate weakness or inability to move the arm. These features suggest an acute complete rotator cuff tear that may benefit from early surgical assessment.
Shoulder pain that has persisted for more than two to three weeks without meaningful improvement despite rest and over-the-counter medications, pain that regularly disrupts sleep, progressive worsening of shoulder pain or weakness, or shoulder pain that significantly limits your ability to work, care for yourself, or participate in activities that matter to you are all sufficient reasons to seek evaluation. A healthcare provider — whether a primary care physician, orthopedic surgeon, or sports medicine specialist — can perform a thorough assessment, arrange appropriate imaging if indicated, and develop a treatment plan tailored to your specific situation and goals. Early evaluation consistently leads to earlier, more effective treatment and better long-term outcomes than prolonged delay.
Conclusion
Rotator cuff pain is a common, complex, and sometimes chronic condition that affects people across all walks of life. Understanding its origins, its characteristic patterns, the factors that worsen it, and the full spectrum of available treatments empowers you to respond to it intelligently rather than simply enduring it or avoiding it. The good news is that the vast majority of people with rotator cuff pain — even those with significant structural damage — can achieve meaningful pain relief and functional improvement with appropriate, well-executed management.
The keys to success are: recognizing the problem early, seeking professional evaluation when needed, committing to a comprehensive rehabilitation program, addressing the mechanical and lifestyle factors that contributed to the problem, and maintaining the habits of regular exercise and body awareness that protect the shoulder for the long term. Your shoulder is a remarkable, complex structure — and with the right approach, rotator cuff pain does not have to be a permanent feature of your life.