Rotator Cuff Tear: Types, Causes, and Treatment Options
What Is a Rotator Cuff Tear?
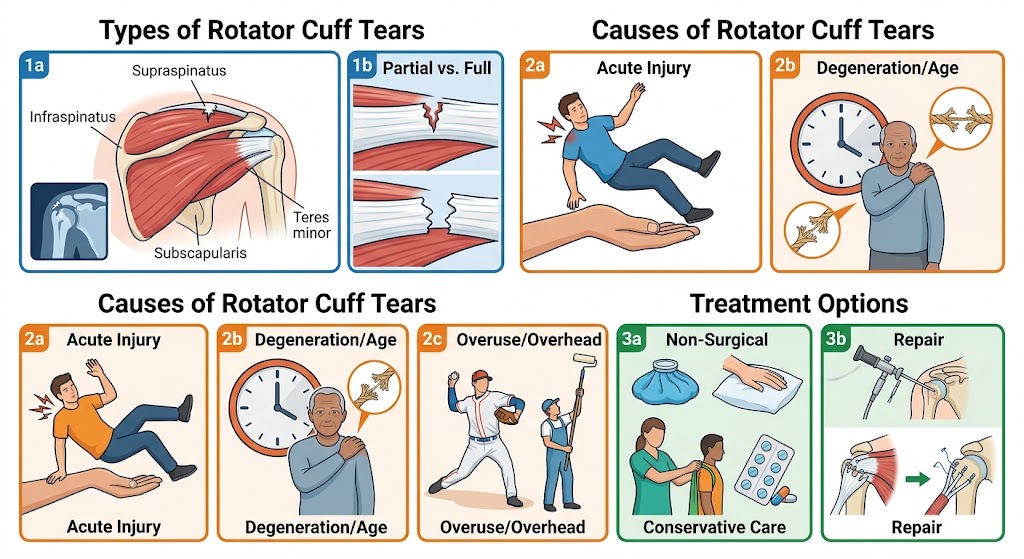
A rotator cuff tear occurs when one or more of the tendons that attach the rotator cuff muscles to the upper arm bone (humerus) become partially or completely severed. The rotator cuff consists of four muscles — supraspinatus, infraspinatus, teres minor, and subscapularis — and their tendons work together to stabilize the shoulder and power arm movements. A tear in any of these tendons compromises both shoulder stability and function.
Rotator cuff tears are among the most common causes of shoulder pain and disability, particularly in adults over the age of 40. They can occur suddenly from an acute injury or develop gradually as a result of chronic overuse and age-related tendon degeneration. Understanding the type and severity of a rotator cuff tear is essential for choosing the right treatment.
Types of Rotator Cuff Tears
Rotator cuff tears are classified in several ways. Based on thickness, tears fall into two main categories: partial-thickness tears, where the tendon is damaged but not completely severed; and full-thickness (complete) tears, where the tendon is completely torn through. Full-thickness tears can be further categorized as small (less than 1 cm), medium (1–3 cm), large (3–5 cm), or massive (greater than 5 cm or involving multiple tendons).
Based on the mechanism of injury, tears are also described as acute (resulting from a sudden traumatic event) or degenerative (developing slowly over time due to wear and tear). Degenerative tears are far more common and account for the vast majority of rotator cuff tear diagnoses.
The supraspinatus tendon is the most frequently torn component of the rotator cuff, as it runs through a narrow space beneath the acromion bone where it is particularly vulnerable to impingement and mechanical wear.

Common Causes of Rotator Cuff Tears
Acute rotator cuff tears typically result from a specific traumatic event. Common mechanisms include falling on an outstretched hand, lifting a very heavy object with sudden force, a direct blow to the shoulder, or forceful pulling or wrenching of the arm. Athletes in overhead sports — pitchers, swimmers, tennis players, and weightlifters — are at elevated risk of acute tears.
Degenerative rotator cuff tears develop over years of repetitive microtrauma. Risk factors include age (most degenerative tears occur in people over 40), occupations requiring repetitive overhead work, smoking (which reduces blood supply to tendons), previous shoulder injuries, and bone spurs that mechanically abrade the tendons over time.
Recognizing a Rotator Cuff Tear
The clinical presentation of a rotator cuff tear depends on whether the tear is acute or degenerative and whether it is partial or complete. Typical symptoms include a dull, aching pain deep in the shoulder that worsens with activity and at night; weakness when attempting to lift or rotate the arm; difficulty reaching overhead or behind the back; and a feeling of the shoulder "giving way" under load.
Interestingly, some large and even massive rotator cuff tears are relatively painless, particularly in older patients whose bodies have adapted to the chronic degenerative process. In contrast, an acute tear is usually accompanied by sudden, severe pain at the time of injury followed by significant weakness and limited mobility.
Diagnosing a Rotator Cuff Tear
Diagnosis begins with a detailed history and physical examination. Orthopedic tests such as the Jobe (empty can) test, drop arm test, Hawkins-Kennedy test, and Gerber lift-off test help identify which tendons are involved and the degree of functional loss.
MRI is the imaging gold standard for evaluating rotator cuff tears, providing detailed information about the size, location, and quality of the remaining tendon tissue (which is critical for surgical planning). Musculoskeletal ultrasound is an excellent, cost-effective alternative that can dynamically assess tendon integrity. X-rays are used to rule out associated bony pathology such as fractures, arthritis, or bone spurs.
Treatment Options for Rotator Cuff Tears
Treatment of rotator cuff tears depends on the size of the tear, the patient's age and activity level, the duration of symptoms, and whether the tear is degenerative or acute.
Non-surgical treatment is appropriate for many partial-thickness tears and for degenerative full-thickness tears in older, less active individuals. This approach includes activity modification, NSAIDs for pain and inflammation, physical therapy focused on strengthening the shoulder muscles and improving biomechanics, and corticosteroid injections for pain relief. Many patients achieve excellent functional outcomes with conservative management alone.
Surgical repair is generally recommended for acute full-thickness tears in younger, active patients; for tears that fail to improve with conservative treatment after 3–6 months; and for large or massive tears causing significant functional disability. Arthroscopic rotator cuff repair is the most common surgical technique, offering smaller incisions, faster recovery, and lower complication rates compared to open surgery.
Recovery After Rotator Cuff Tear Treatment
Recovery timelines vary considerably. After surgical repair, patients typically wear a sling for 4–6 weeks, followed by a structured physical therapy program lasting 4–6 months before returning to full activity. Full recovery and return to sport or demanding physical work may take 9–12 months for large tears.
Non-surgical recovery is generally faster for small tears — most patients see significant improvement within 3–6 months of consistent physical therapy. However, non-surgically treated tears may not heal completely, and there is a risk of tear progression over time, particularly with continued physical demands.
When Surgery Is the Best Choice
The decision to pursue surgical repair should be made collaboratively between the patient and an orthopedic surgeon. Surgery is particularly favored for young, active patients with acute full-thickness tears, as repaired tendons heal most predictably in this population. Delaying surgery in such cases can allow the torn tendon ends to retract and the muscle to atrophy, making successful repair progressively more difficult.
Conclusion
A rotator cuff tear is a serious but treatable injury. Whether managed conservatively or surgically, the majority of patients achieve meaningful pain relief and functional recovery with appropriate care. Early diagnosis, a thorough understanding of the tear type, and a commitment to rehabilitation are the pillars of a successful outcome.