Symptoms of Rotator Cuff Tear: A Detailed Clinical Overview
Introduction to Symptoms of Rotator Cuff Tear
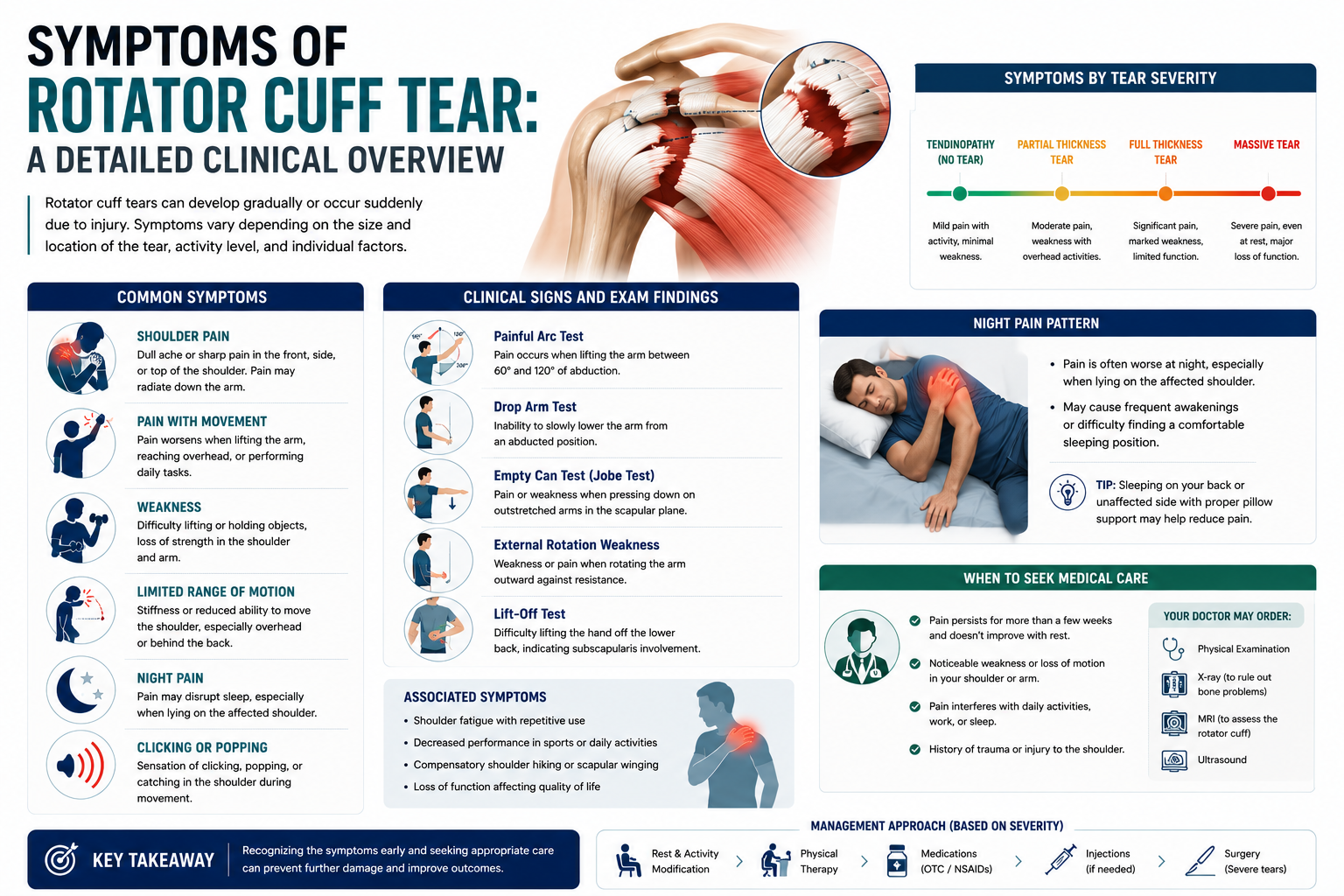
The symptoms of rotator cuff tear vary widely depending on the type of tear, its size, which tendon is affected, and whether the injury occurred suddenly or developed over time. Because these symptoms can mimic those of other shoulder conditions — including shoulder impingement, bursitis, and biceps tendinitis — a thorough understanding of the full clinical picture is essential for accurate self-assessment and proper medical diagnosis.
This article provides a detailed clinical overview of the symptoms of rotator cuff tear, organized by symptom type, severity, and clinical significance.
Pain Patterns in Rotator Cuff Tears
Pain is the most universal symptom of rotator cuff tear. It is typically located along the outer aspect of the shoulder and upper arm, often described as a deep, aching discomfort that is difficult to localize precisely. Pain may radiate down the lateral (outer) upper arm to the level of the elbow, but rarely extends below the elbow — an important distinction from cervical radiculopathy, where pain and numbness may radiate all the way to the hand.
Pain intensity and character can vary. Acute tears (resulting from a traumatic event such as a fall or sudden forceful movement) typically produce immediate, sharp, intense pain at the moment of injury, followed by a persistent dull ache. Degenerative tears (developing gradually over time) often begin with intermittent, activity-related discomfort that progressively becomes more constant and more severe as the tear enlarges.

Provocative activities that worsen pain include overhead reaching, lateral arm raises against resistance, reaching behind the back, carrying heavy objects with the arm extended, and any activity requiring sustained shoulder rotation. Pain typically improves with rest, though it may not fully resolve.
Night Pain and Sleep Disturbance
Night pain is one of the most clinically significant symptoms of rotator cuff tear and is present in the majority of patients with symptomatic tears. Pain is typically worst when lying on the affected shoulder, but many patients also report pain lying on their back with the arm at the side or lying on the opposite side. The mechanism involves increased mechanical pressure on the compromised tendon when the shoulder is in a relaxed, unloaded position, combined with reduced distraction from pain during quiet periods.
Chronic sleep disruption due to shoulder pain is associated with increased fatigue, irritability, reduced quality of life, and can exacerbate pain sensitivity — making it an important target of both conservative and surgical treatment.
Weakness and Functional Loss
Shoulder weakness is a particularly important symptom of rotator cuff tear because it reflects the extent of structural disruption. Different patterns of weakness point to different tendons being affected. Supraspinatus tears produce weakness with shoulder abduction (lifting the arm out to the side) and forward flexion. Infraspinatus tears cause weakness with external rotation (turning the arm outward), such as when throwing or steering. Subscapularis tears result in weakness with internal rotation (turning the arm inward), such as reaching behind the back.
For partial tears, weakness may be subtle — patients notice it mainly during demanding activities like throwing or lifting weights. For full-thickness tears, weakness can be severe enough to make basic daily tasks like dressing, hair washing, and reaching overhead impossible without assistance.
Restricted Range of Motion
While pain is the dominant presenting symptom, restriction of shoulder movement frequently accompanies rotator cuff tears. Active range of motion (movements the patient initiates) is typically more restricted than passive range of motion (movements performed by an examiner), reflecting the muscular component of the loss. The most commonly restricted planes of movement are forward flexion (raising the arm in front), abduction (raising to the side), and internal rotation (reaching behind the back).
In patients with longstanding, untreated tears, secondary stiffening of the shoulder capsule can develop, leading to adhesive capsulitis. This superimposed condition further limits both active and passive range of motion and significantly complicates treatment and rehabilitation.
Crepitus, Clicking, and Mechanical Symptoms
Audible or palpable mechanical symptoms during shoulder movement are frequently reported by patients with rotator cuff tears. These include clicking or popping sensations during arm elevation, a catching feeling at specific points in the motion arc, grinding or crepitus during shoulder rotation, and in some cases, a sense of the shoulder "giving way" under load. These mechanical symptoms arise from torn tendon edges catching on adjacent structures, irregular joint mechanics due to disrupted stabilization, and degenerative changes in the joint secondary to the tear.
Muscle Atrophy
In chronic or large rotator cuff tears, visible muscle wasting may develop, particularly in the supraspinatus and infraspinatus fossae (the areas above and below the spine of the scapula on the back of the shoulder). This atrophy indicates prolonged disuse or denervation of the affected muscles and has significant implications for treatment: muscles that have atrophied extensively may not fully recover function even after successful surgical repair, making early treatment particularly important.
Acute vs. Chronic Symptom Presentation
The temporal pattern of symptom onset provides important diagnostic information. An acute rotator cuff tear in an otherwise healthy tendon (typically in younger patients) produces immediate, severe pain with rapid onset of weakness and functional loss. The shoulder is visibly distressed and movement is severely guarded. A chronic or degenerative tear develops over months to years, with symptoms that begin subtly and gradually worsen. Paradoxically, some patients with large chronic tears report surprisingly little pain — having adapted over time — but significant functional loss and weakness.
Diagnosis: Turning Symptoms into a Diagnosis
When symptoms of rotator cuff tear are present, a structured clinical evaluation begins with orthopedic tests designed to stress specific tendons. The empty-can (Jobe) test assesses the supraspinatus; the lift-off and belly-press tests evaluate the subscapularis; the external rotation lag sign and infraspinatus test assess external rotation strength. Positive findings on multiple tests increase diagnostic specificity. MRI or musculoskeletal ultrasound confirms the diagnosis and characterizes the tear for treatment planning.
Conclusion
The symptoms of rotator cuff tear constitute a recognizable clinical syndrome centered on shoulder pain (especially at night), progressive weakness, and restricted movement. The more symptoms are present — and the more severe they are — the larger and more significant the underlying tear is likely to be. If you recognize these symptoms, seek orthopedic evaluation promptly. Early diagnosis leads to better treatment options and better outcomes.