Torn Rotator Cuff: Everything You Need to Know
What Is a Torn Rotator Cuff?
A torn rotator cuff is one of the most significant and common shoulder injuries affecting people worldwide. It occurs when one or more of the four tendons of the rotator cuff — the supraspinatus, infraspinatus, teres minor, or subscapularis — are partially or completely ruptured. These tendons attach the rotator cuff muscles to the head of the humerus (upper arm bone) and are essential for shoulder stability and the ability to lift, reach, and rotate the arm.
Rotator cuff tears affect people of all ages and activity levels, though they are most prevalent in adults over 40. They can result from a single traumatic event or from years of gradual degeneration. Understanding the full scope of this injury — from its causes and symptoms to its diagnosis, treatment, and prognosis — is essential for anyone dealing with shoulder pain or functional loss.
Anatomy of the Rotator Cuff
To understand a torn rotator cuff, it helps to appreciate the anatomy it involves. The rotator cuff consists of four muscles that originate on the scapula (shoulder blade) and insert via tendons onto the humerus. Together, they form a "cuff" of tissue surrounding the shoulder joint. The supraspinatus is the most commonly torn tendon, running beneath the acromion bone where it is vulnerable to impingement and wear. The infraspinatus and teres minor drive external rotation. The subscapularis is the only muscle on the anterior (front) face of the scapula and controls internal rotation. All four work together to dynamically stabilize the shoulder and power arm movements.
Types of Rotator Cuff Tears

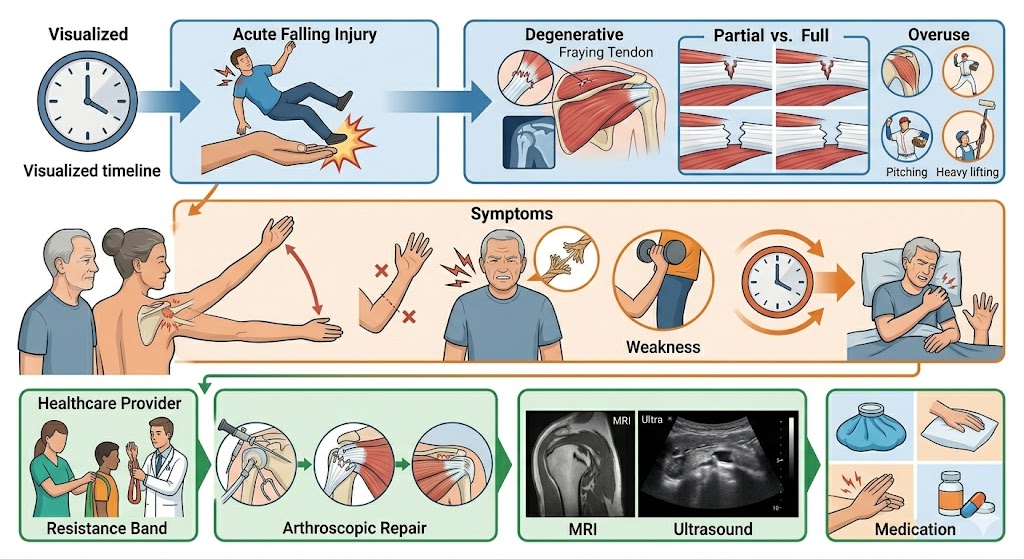
Rotator cuff tears are classified by thickness and by the mechanism of injury. Partial-thickness tears involve damage to part of the tendon, which is not completely severed. These can be articular-side (facing the joint), bursal-side (facing the subacromial bursa), or intratendinous (within the substance of the tendon). Full-thickness tears — where the tendon is completely ruptured from top to bottom — are further described by size: small (less than 1 cm), medium (1–3 cm), large (3–5 cm), and massive (more than 5 cm, or involving two or more tendons).
By mechanism, tears are either acute (sudden traumatic onset) or degenerative (gradual chronic wear). Degenerative tears are far more common, accounting for the majority of rotator cuff tear diagnoses, particularly in patients over 50.
Causes of a Torn Rotator Cuff
The most common cause of a torn rotator cuff in younger patients is acute trauma — a fall on an outstretched arm, a sudden forceful pull of the arm, a shoulder dislocation, or a direct blow. The forces involved exceed the tensile strength of the tendon, causing immediate rupture.
In older patients, degenerative changes are the primary driver. Over decades of use, the rotator cuff tendons undergo microscopic fiber disruption, reduced collagen organization, decreased vascularity (blood supply), and mechanical impingement under the acromion bone. This progressive deterioration weakens the tendon until normal daily activities — reaching overhead, lifting a bag, or rolling over in bed — can precipitate a full tear in already compromised tissue.
Risk factors include age over 40, repetitive overhead occupational or athletic activity, smoking, a history of previous shoulder injury or surgery, and the presence of bone spurs beneath the acromion that mechanically abrade the tendons over time.
Symptoms of a Torn Rotator Cuff
A torn rotator cuff produces a constellation of symptoms that, while variable in severity, follow a recognizable pattern. Shoulder pain — typically a deep, aching discomfort on the lateral or anterior shoulder — is the most universal symptom. Pain is provoked by overhead activities, lifting, and shoulder rotation, and is notably worse at night, often waking patients from sleep.
Weakness is a defining feature: patients struggle to lift the arm, hold it in an elevated position, or rotate it against resistance. The severity of weakness correlates roughly with the size of the tear. Restricted range of motion frequently accompanies pain and weakness, particularly with forward elevation, abduction, and internal rotation (reaching behind the back). Mechanical sensations — clicking, catching, or a grinding crepitus — are also commonly reported.
In massive tears, the arm may be entirely unable to be actively raised despite passive motion being preserved — a phenomenon known as pseudoparalysis, which represents one of the most severe functional consequences of rotator cuff pathology.
Diagnosing a Torn Rotator Cuff
Diagnosis begins with a clinical evaluation by a physician or orthopedic specialist. Key orthopedic tests — the Jobe (empty can) test, drop arm test, Hawkins-Kennedy test, external rotation lag sign, and Gerber lift-off test — help identify which tendons are compromised and the degree of functional loss. The clinical picture is then confirmed with imaging.
MRI (magnetic resonance imaging) is the gold standard for evaluating a torn rotator cuff, providing detailed information about the size, location, depth, tendon retraction, and muscle quality of the tear — all critical factors for surgical planning. Musculoskeletal ultrasound offers a real-time, cost-effective alternative with excellent accuracy for detecting tears. X-rays are used to rule out associated bony pathology such as fractures, glenohumeral arthritis, or subacromial bone spurs.
Treatment of a Torn Rotator Cuff
Treatment decisions for a torn rotator cuff depend on multiple factors: the patient's age, activity level, and functional demands; the size and type of the tear; symptom severity; and whether the tear is acute or degenerative.
Conservative (non-surgical) treatment is appropriate for many partial tears and for degenerative full-thickness tears in older, lower-activity patients. It includes activity modification, NSAIDs for pain and inflammation, physical therapy focused on rotator cuff strengthening and shoulder biomechanics correction, and corticosteroid injections for pain management. Many patients achieve satisfactory functional recovery with conservative care alone.
Surgical repair is recommended for acute full-thickness tears in younger, active patients; for partial tears that fail to improve after 3–6 months of conservative treatment; for full-thickness tears causing significant functional impairment; and for patients whose activities demand full shoulder strength and stability. Arthroscopic rotator cuff repair is the modern standard of care, offering smaller incisions, direct visualization, and faster recovery compared to open repair techniques.
Recovery and Rehabilitation
Recovery from a torn rotator cuff — whether treated conservatively or surgically — is a process that requires patience and commitment to rehabilitation. After surgical repair, patients typically wear a sling for 4–6 weeks, followed by a phased physical therapy program. Range of motion exercises begin early, followed by progressive strengthening at 3–4 months post-surgery. Return to sport or heavy physical work generally occurs at 9–12 months for large or massive tears.
Non-surgical recovery is faster for small tears, with most patients experiencing significant improvement within 3–6 months of consistent therapy. However, some conservative cases — particularly those involving full-thickness tears — remain symptomatic long term and may eventually require surgery. Monitoring and ongoing exercise are important even after successful conservative management.
Prognosis: What to Expect Long Term
The prognosis for a torn rotator cuff depends on the size of the tear, the treatment chosen, the patient's adherence to rehabilitation, and pre-existing factors such as muscle atrophy and fatty infiltration. Small to medium tears that are repaired early in appropriate candidates carry excellent prognoses, with most patients achieving significant pain relief and functional recovery. Massive or neglected tears with severe muscle atrophy carry a guarded prognosis, as muscle recovery may be incomplete even after successful tendon repair.
Degenerative tears managed conservatively in elderly patients often achieve good pain relief and functional improvement with physical therapy, even without surgical repair. The key is individualized treatment tailored to the patient's needs, goals, and tear characteristics.
Conclusion
A torn rotator cuff is a serious but highly manageable shoulder injury. With accurate diagnosis, appropriate treatment selection — whether conservative or surgical — and dedicated rehabilitation, the overwhelming majority of patients can achieve meaningful recovery of pain, strength, and shoulder function. If you suspect a torn rotator cuff, do not delay seeking evaluation. The sooner it is diagnosed and treated, the better your outcome is likely to be.